Early Detection
Early detection allows more effective treatment when the cancer is at an earlier, much more curable stage.
Detection of some cancers at an early stage combined with prompt treatment permits less aggressive treatment, leading to a better quality of life of the patient, and is associated with significantly reduced mortality. There are two distinct approaches to early detection—screening and early diagnosis.
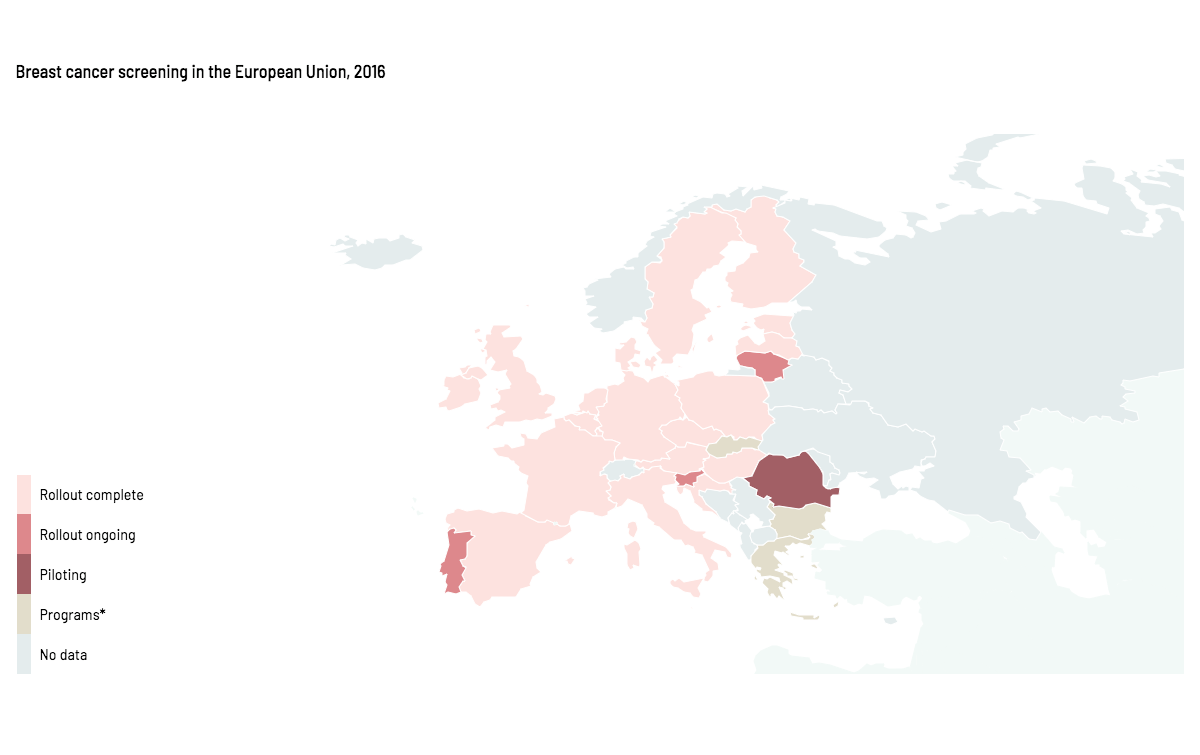
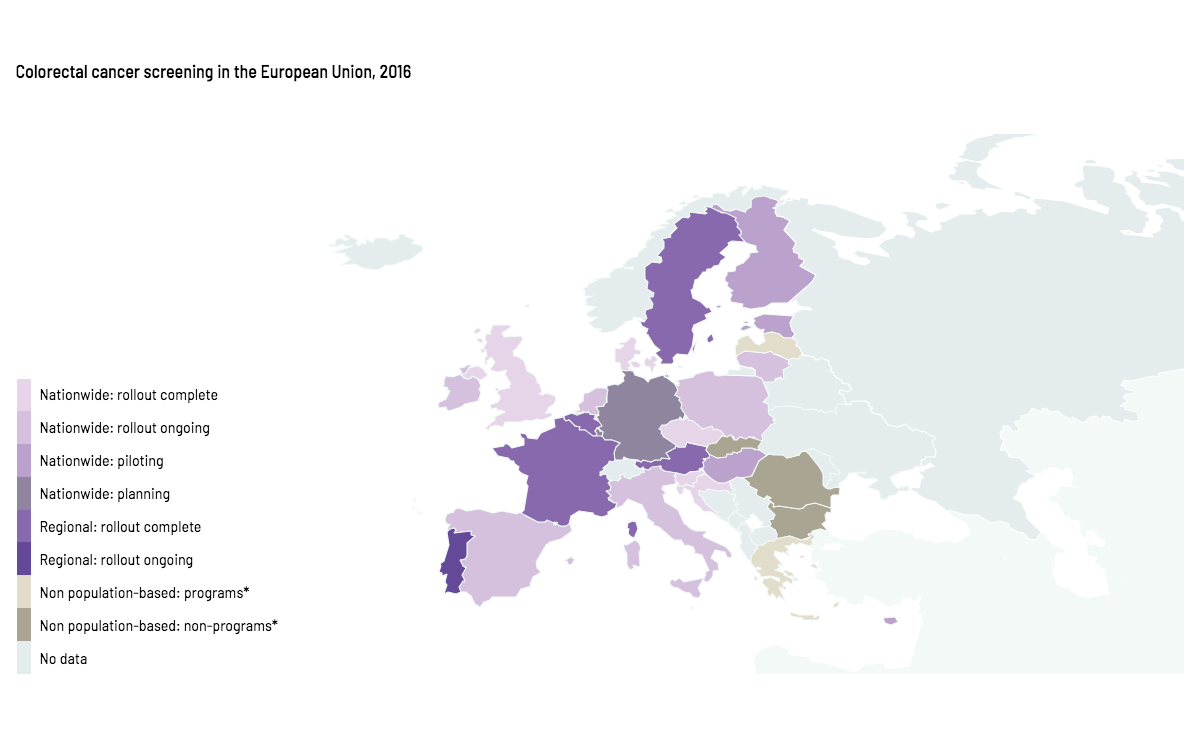
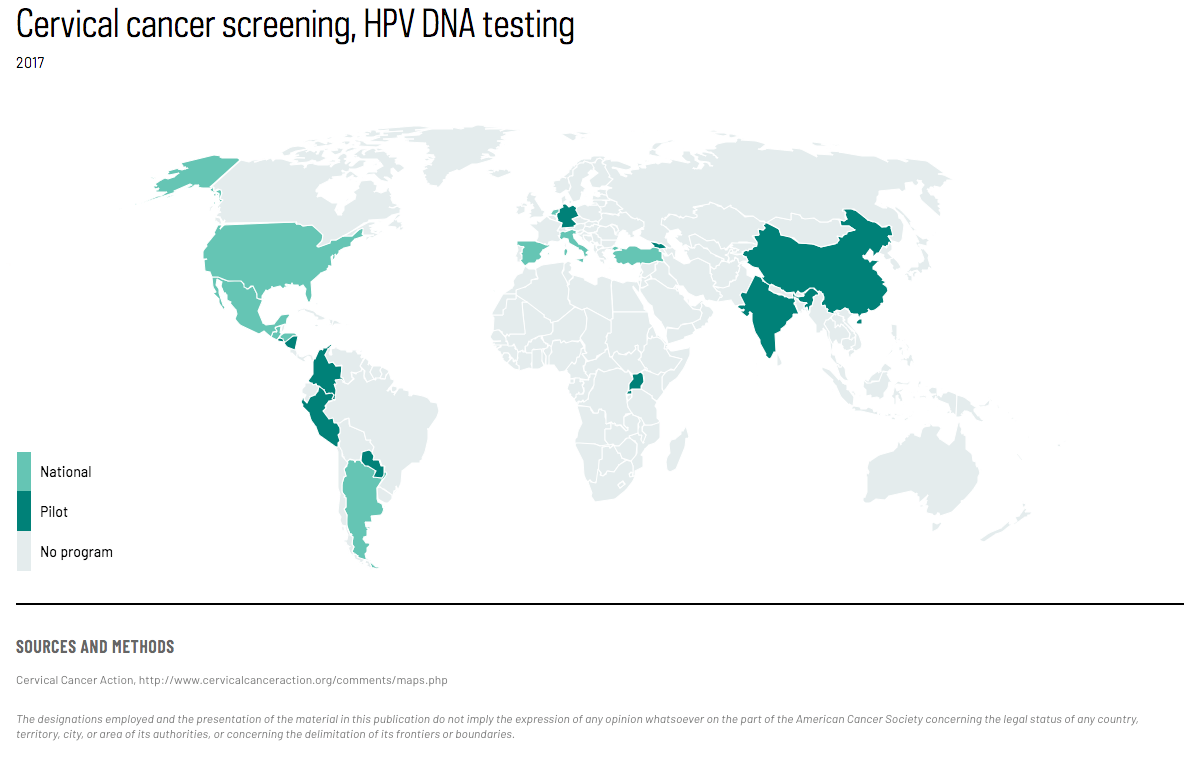
Screening involves systematic examination of an apparently healthy and asymptomatic population at risk with a test to detect the disease at an early stage. However, implementation is quite complex and resource-intensive. Screening may be population-based (inviting the entire target population at the appropriate intervals) or opportunistic (at the initiation of the patient or upon invitation at an unrelated clinical encounter). To date, screening of the general population is recommended only for cervical, colorectal, and female breast cancer, depending on resources of the country. (Map 1–3)
{kind=link}
ACCESS CREATES PROGRESS
Programs to raise awareness of breast cancer and promote clinical breast examination in countries where mammography screening is not feasible have resulted in more breast cancers being diagnosed at an early stage.
{kind=link}
{kind=link}
Oral cancer screening is recommended for habitual users of tobacco or alcohol. Lung cancer screening is recommended in the United States for current and former heavy smokers aged 55–74 years. In addition to detection at an early stage, screening can prevent cervical and colorectal cancers through detection and removal of premalignant conditions. (Figure 1)
Figure 1. Decreases in cervical cancer incidence rates between 1960–2016, age-standardized rate (world) per 100,000.
Cervical cancer incidence rates in Denmark decreased from 31 cases per 100,000 in 1960 to 9 in 2016.
Cervical cancer incidence rates in Sweden decreased from 16 cases per 100,000 in 1960 to 9 in 2016.
Cervical cancer incidence rates in Norway decreased from 16 cases per 100,000 in 1960 to 10 in 2016.
Cervical cancer incidence rates in Finland decreased from 14 cases per 100,000 in 1960 to 4 in 2016.
Cervical cancer incidence rates in the United States (SEER 9 registries) decreased from 12 cases per 100,000 in 1975 to 5 in 2016.
Early diagnosis is detection of a cancer at the earliest possible stage, usually through patient awareness of the early symptoms of common cancers, and training of healthcare workers to recognize and appropriately refer patients with probable early cancer symptoms. (Figure 2) While not as effective as screening, it can be used for many of the most common cancers including breast, skin, and stomach, and in low-resource settings where screening may not be feasible. Early diagnosis is an important component of any early detection program because not all adults are invited to screening or attend screening, and screening programs fail to detect some cancers.
Population awareness, trained healthcare providers, prompt referral systems, and diagnostic and therapeutic infrastructure are necessary for both screening and early diagnosis to function well.
Cervical cancer death rates in high income countries:
International Agency for Research on Cancer. IARC Handbooks of Cancer Prevention volume 10: Cervix Cancer Screening. Lyon: IARC, 2005.
Access creates progress:
Denny L, de Sanjose S, Mutebi M, et al. Interventions to close the divide for women with breast and cervical cancer between low-income and middle-income countries and high-income countries. Lancet. 2017;389:861–870.
Text:
Arbyn M, Anttila A, Jordan J, Ronco G, Schenck U, Segnan N, Wiener HG, Herbert A, Daniel J, von Karsa L. European guidelines for quality assurance in cervical cancer screening. Second edition. Luxembourg: European Union, 2008.
Dobrow MJ, Hagens V, Chafe R, Sullivan T, Rabeneck L. Consolidated principles for screening based on a systematic review and consensus process. CMAJ. 2018;190(14):E422-E429.
Ferlay J, Colombet M and Bray F. Cancer Incidence in Five Continents, CI5plus: IARC CancerBase No. 9 [Internet]. Lyon, France: International Agency for Research on Cancer; 2018. Available from: http://ci5.iarc.fr.
IARC. IARC Handbooks of Cancer Prevention Volume 15. Breast Cancer Screening. Lyon: International Agency for Research on Cancer, 2016.
Marmot MG, Altman DG, Cameron DA, Dewar JA, Thompson SG, Wilcox M. The benefits and harms of breast cancer screening: an independent review. Br J Cancer. 2013;108(11):2205–40.
Moyer VA; U.S. Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330–8.
Park S, Oh CM, Cho H, Lee JY, Jung KW, Jun JK, Won YJ, Kong HJ, Choi KS, Lee YJ, Lee JS. Association between screening and the thyroid cancer “epidemic” in South Korea: evidence from a nationwide study. BMJ. 2016;355:i5745.
Segnan N, Patnick J, von Karsa L. European guidelines for quality assurance in colorectal cancer screening and diagnosis. First edition. Luxembourg: European Union, 2010.
WHO. Guide to cancer early diagnosis. Geneva: World Health Organization, 2017.
Wilson JMG, Jungner G. Principles and practice of screening for disease. Geneva: World Health Organization, 1968.
World Health Organization. Department of Information. Evidence and Research. Mortality database. Available from: http://www-dep.iarc.fr/WHOdb/WHOdb.htm
Maps 1 and 2:
Used with permission under copyright from John Wiley and Sons: Basu P, Ponti A, Anttila A, et al. Status of implementation and organization of cancer screening in The European Union Member States-Summary results from the second European screening report. Int J Cancer. 2018;142:44–56.
Map 3:
Cervical Cancer Action. Global progress in cervical cancer prevention. http://www.cervicalcanceraction.org/comments/maps.php
Figure 1:
Cancer Control Knowledge into Action: WHO Guide for Effective Programs. Early Detection. 2007. https://www.who.int/cancer/modules/Early%20Detection%20Module%203.pdf
Figure 2:
Danckert B, Ferlay J, Engholm G , et al. NORDCAN: Cancer Incidence, Mortality, Prevalence and Survival in the Nordic Countries, Version 8.2 (26.03.2019).
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence – SEER 9 Regs Research Data, Nov 2018 Sub (1975–2016) <Katrina/Rita Population Adjustment> – Linked To County Attributes – Total U.S., 1969–2017 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2019, based on the November 2018 submission.