Environmental & Occupational Exposures
Limiting carcinogenic exposures in the environment and in the workplace provides an opportunity to reduce the cancer burden, particularly for workers with unacceptably high exposures.
ENVIRONMENTAL POLLUTANTS
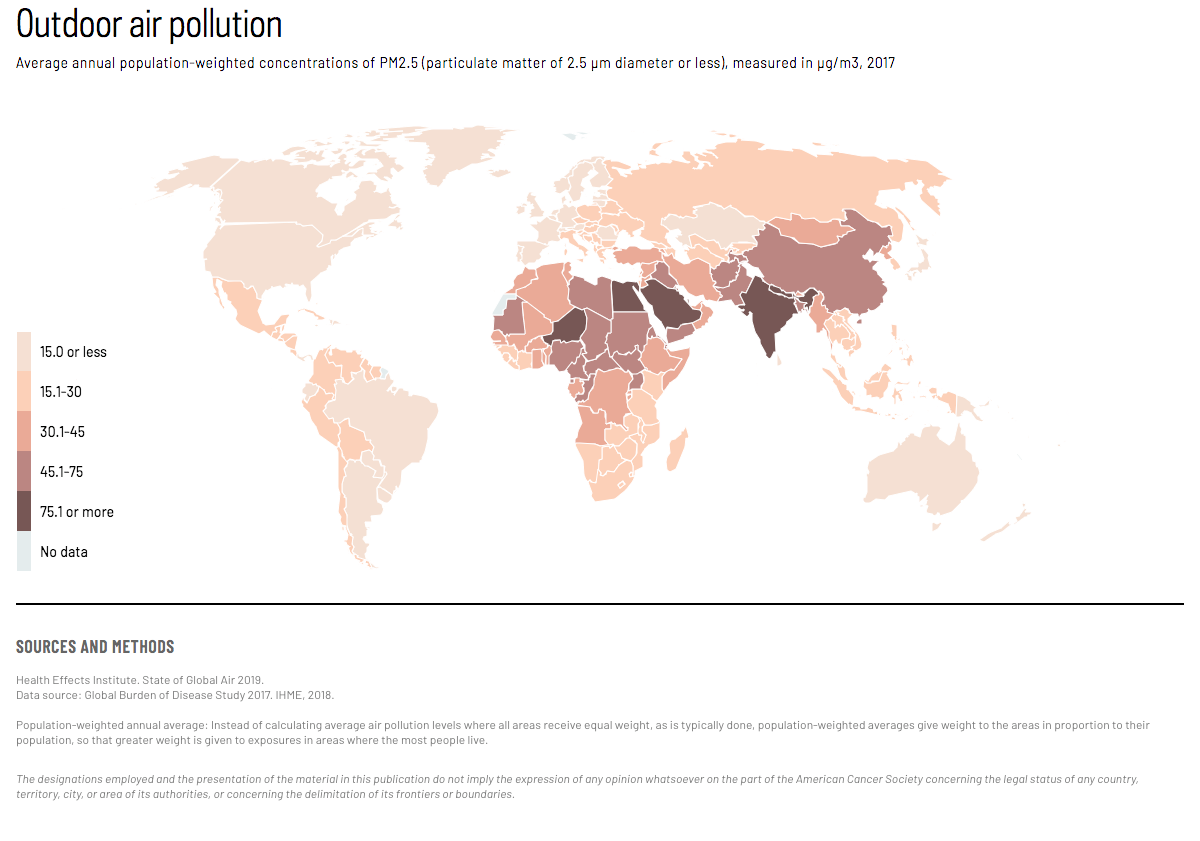
Outdoor air pollution causes between 6 and 8 million premature deaths from lung cancer and other diseases each year. The International Agency for Research on Cancer (IARC) has classified outdoor air pollution and the particulate matter in outdoor air pollution as known human carcinogens. Outdoor air pollution levels are particularly high in rapidly-growing cities in low- and middle-income countries. (Map 1) Diesel exhaust, also classified as a lung carcinogen by IARC, contributes to outdoor air pollution and is also an occupational lung carcinogen.
The air we breathe has become polluted with a mixture of cancer-causing substances. We now know that outdoor air pollution is not only a major risk to health in general, but also a leading environmental cause of cancer deaths.
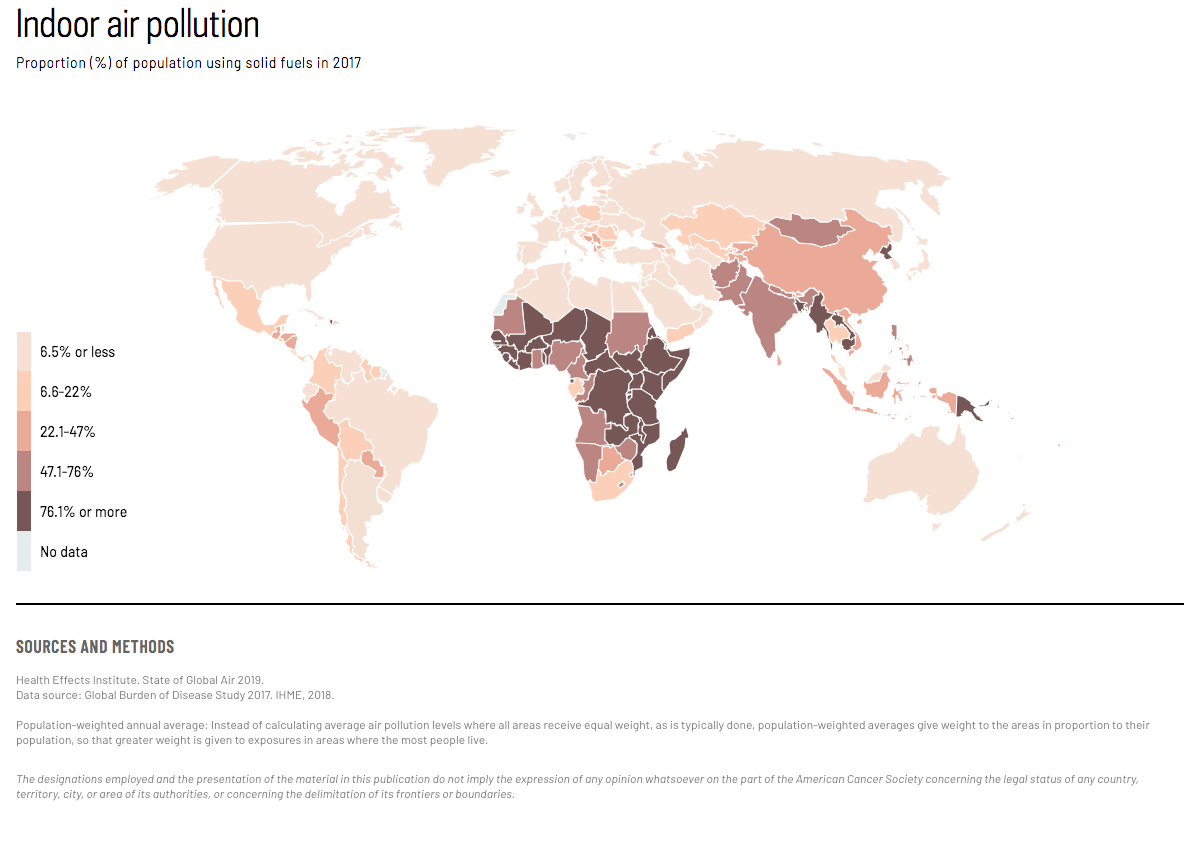
Indoor air pollution from use of solid fuel (e.g. wood, other biomass, and coal) is estimated to cause about 3.8 million deaths, including about 285,000 lung cancer deaths, each year in low- and middle-income countries. Globally, the number of people cooking with solid fuels has declined, but populations in less-developed countries continue to be exposed to high levels of household air pollution. (Map 2, Figure 1) IARC classifies indoor smoke emissions from coal as a known human carcinogen, and from other types of solid fuels as probable carcinogens.
Figure 1. Proportion (%) of population using solid fuels, 1990-2017. Solid fuel use in sub-Saharan Africa has remained around 80% from 1990-2017. Solid fuel use in South Asia has declined from around 85% in 1990 to 61% in 2017. Solid fuel use in Southeast Asia, East Asia, and Oceania has declined from around 75% in 1990 to 38% in 2017. Solid fuel use in Latin America and Caribbean has declined from around 35% in 1990 to 16% in 2017. Solid fuel use in North Africa and Middle East has declined from around 25% in 1990 to 15% in 2017. Solid fuel use in Central Europe, Eastern Europe, and Central Asia has declined from around 20% in 1990 to 10% in 2017.
Exposure to radon is probably the second-leading cause of lung cancer in the United States and Europe. Radon gas forms from the radioactive decay of uranium, found at differing concentrations in soil and rock throughout the world. While the general population is exposed primarily from radon gas entering homes from the soil, exposure to high levels of radon can also occur when the gas is trapped in underground mines.
Populations consuming high levels of arsenic in drinking water have excess risks of skin, lung, and bladder cancer. High levels of arsenic in drinking water have been found in parts of China, Bangladesh, and some countries in Central and South America. Some predominantly occupational exposures, such as asbestos and asbestiform fibers, benzene, and polychlorinated biphenyls (PCBs), may also occur in the general population, albeit at lower levels.
OCCUPATIONAL EXPOSURES
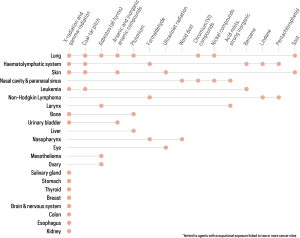
Numerous substances are known to cause cancer in workers. (Figure 2) Due to the intensity and/or duration of these exposures, the cancer burden can be relatively high among those workers exposed. Exposure to occupational carcinogens remains a concern in low- and middle-income countries, where exposures are likely to be higher than in high-income countries, and regulations and enforcement are often less strict.
{kind=link}
{kind=link}
*Limited to agents with occupational exposure linked to two or more cancer sites. X-radiation and gamma-radiation are associated with cancers of the lung; hemolymphatic system; skin; leukemia; bone; urinary bladder; salivary gland; stomach; thyroid; breast; brain and nervous system; colon; esophagus; and kidney. Coal-tar pitch is associated with cancers of the lung; hemolymphatic system; skin; and leukemia. Asbestos (all forms) is associated with cancers of the lung; larynx; mesothelioma; and ovary. Arsenic and inorganic arsenic compounds are associated with cancers of the lung; skin; and urinary bladder. Plutonium is associated with cancers of the lung; bone; and liver. Formaldehyde is associated with cancers of the hemolymphatic system; non-Hodgkin lymphoma; and nasopharynx. Ultraviolet radiation is associated with cancers of the skin and eye. Wood dust is associated with cancers of the nasal cavity and paranasal sinus and nasopharynx. Chromium (VI) compounds are associated with cancers of the lung and nasal cavity and paranasal sinus. Nickel compounds are associated with cancers of the lung and nasal cavity and paranasal sinus. Acid mists, strong inorganic are associated with cancers of the nasal cavity and paranasal sinus and larynx. Benzene is associated with cancers of the hemolymphatic system and leukemia. Lindane is associated with cancers of the hemolymphatic system and non-Hodgkin lymphoma. Pentachlorophenol is associated with cancers of the hemolymphatic system and non-Hodgkin lymphoma. Soot is associated with cancers of the lung and skin.
Asbestos is an important cause of occupational lung cancer and the unique cause of malignant mesothelioma, and remains an occupational and environmental hazard in many countries. However, there are many other causes of occupational cancer, and asbestos accounts for less than one-third of occupational cancers globally.
Outdoor air pollution exposure:
World Health Organization. Global Health Observatory data repository. https://www.who.int/gho/en/. Accessed April 24, 2019.
Percent of cancers worldwide attributed to occupational exposure:
Driscoll T, Takala J, Steenland K, Corvalan C, Fingerhut M. Review of estimates of the global burden of injury and illness due to occupational exposures. Am J Ind Med. 2005;48: 491–502.
Rushton L, Hutchings SJ, Fortunato L, et al. Occupational cancer burden in Great Britain. Br J Cancer. 2012;107 Suppl 1: S3-7.
Text:
Loomis D, Guha N, Straif K. Identifying occupational carcinogens: An update from the IARC Monographs. Occupational Environ Med. 2018;75:593-603.
World Health Organization Global Health Observatory Data Repository, http://apps.who.int/gho/data/node.home.
Maps 1–2, and Figure 1:
Health Effects Institute. State of Global Air 2019.
Data source: Global Burden of Disease Study 2017. IHME, 2018.
Population-weighted annual average: Instead of calculating average air pollution levels where all areas receive equal weight, as is typically done, population-weighted averages give weight to the areas in proportion to their population, so that greater weight is given to exposures in areas where the most people live.
Figure 2:
Loomis D, Guha N, Straif K. Identifying occupational carcinogens: an update from the IARC Monographs. Occupational Environ Med. 2018;75:593–603.