The Cancer Continuum
An Overview of Interventions and Potential for Impact: Resource-appropriate, broad application of known interventions in each country can substantially reduce the morbidity and mortality associated with cancer.
Evidence-based, resource appropriate interventions for cancer prevention and control exist across the cancer continuum in each country, from prevention of risk factors to early detection, treatment, survivorship, and end-of-life care. (Figure 1)
Tobacco use, the cause of the largest number of preventable cancers worldwide, can be substantially reduced through raising excise tax on tobacco products, smoke-free air laws, health warnings on tobacco packaging, and restrictions on promotion and advertising of tobacco products. (Figure 2a & b; also see Tobacco Control)Figure 2a. PREVENTION: Cumulative probability (%) of death from lung cancer by attained age and smoking status, male.
Male never smokers have a 1.4% chance of dying of lung cancer by the age of 85. Male smokers who quit by age 40 have a 3.6% chance of dying of lung cancer by the age of 85. Male smokers who quit between age 40-49 have a 7% chance of dying of lung cancer by the age of 85. Male smokers who quit between age 50-59 have an 11.5% chance of dying of lung cancer by the age of 85. Male smokers who quit between age 60-69 have a 19.1% chance of dying of lung cancer by the age of 85. Male smokers who quit by age 70 or older have a 22.7% chance of dying of lung cancer by the age of 85. Male smokers who continue to smoke have a 28.4% chance of dying of lung cancer by the age of 85.
Figure 2b. PREVENTION: Cumulative probability (%) of death from lung cancer by attained age and smoking status, female.
Female never smokers have a 1.1% chance of dying of lung cancer by the age of 85. Female smokers who quit by age 40 have a 1.9% chance of dying of lung cancer by the age of 85. Female smokers who quit between age 40-49 have a 4.9% chance of dying of lung cancer by the age of 85. Female smokers who quit between age 50-59 have a 7.7 % chance of dying of lung cancer by the age of 85. Female smokers who quit between age 60-69 have a 13.7% chance of dying of lung cancer by the age of 85. Female smokers who quit by age 70 or older have a 15% chance of dying of lung cancer by the age of 85. Female smokers who continue to smoke have a 21.3% chance of dying of lung cancer by the age of 85.
Unhealthy diet and physical inactivity can be reduced through increased public awareness about their health hazards and through public policies (e.g., excise tax on sweetened beverages) and structural and environmental interventions (e.g., pedestrian and bike lanes) (see Health Promotion). The hepatitis B virus (HBV) and human papillomavirus (HPV), infections that cause liver cancer (HBV) and cervical and other urogenital and oropharyngeal cancers (HPV), can be prevented through vaccination (see Vaccines).
Indoor and outdoor air pollution can be reduced through use of clean stoves, cleaner fuels, and proper ventilation, and air quality guidelines and policies. Protection from harmful sun exposure could reduce the risk of skin cancer. Cancer-causing occupational exposures could be prevented through improved work place safety. Addressing cancer risk factors can also have a shared impact on other non-communicable diseases.
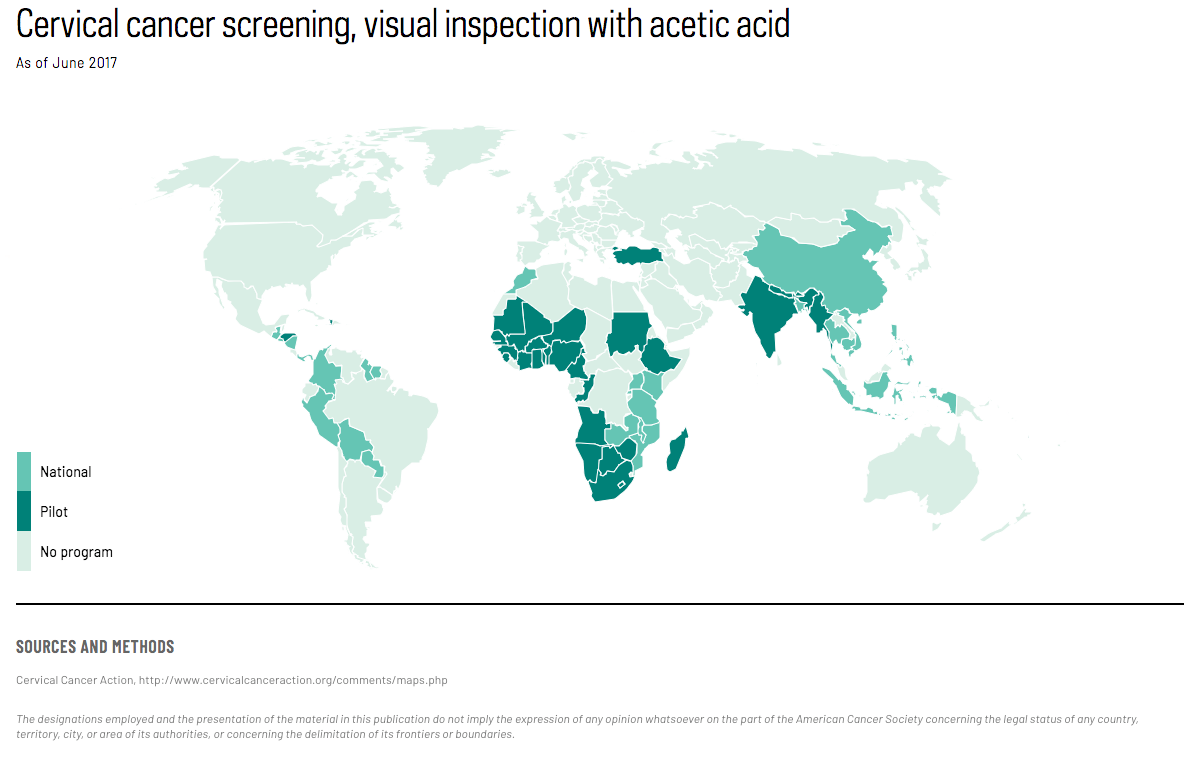
Regular screening for cervical, colorectal, breast, and lung cancers allows detection of these diseases at an early stage, when treatments are more successful and the chance for survival and cure is high. (Map 1)
{kind=link}
Screening for colorectal and cervical cancers also prevents cancer by detecting precancerous lesions for removal by surgery or other forms of treatment. A heightened awareness of warning signs for cancer of the oral cavity, skin, and some other cancers may also lead to detection of cancers at early stage (see Early Detection).
Effective treatment modes (surgery, radiation, chemotherapy, hormonal therapy, immunotherapy) have been developed for several cancers, including for cancers of the breast, colon and rectum, and testis and for many childhood cancers. (Figure 3; also see Management and Treatment) For certain cancers such as testis, treatment could lead to cure, even for advanced-stage disease. Awareness and availability of services to meet the needs of cancer survivors are increasing worldwide (Figure 4), and pain associated with cancer can be controlled by administration of analgesic drugs. (Figure 5; also see Pain Control)
Figure 3. TREATMENT: Childhood cancer mortality trends, all cancer sites combined, males 0–19 years, 1975–2013. Age-standardized rate (world) per 100,000. Childhood cancer mortality rates in Japan and the United States have declined from about 6 in 1975 to about 2 in 2013. Childhood cancer mortality rates in Egypt, Colombia, and Brazil have remained around 5-6 during the same period.
Monitor for long-term conditions
Screening for high-risk cancers
Figure 5. END-OF-LIFE CARE: Adult palliative care needs at the end of life by disease (%) worldwide, 2011. Worldwide palliative care needs at the end of life are comprised of cancer (34%), cardiovascular diseases (38%), chronic obstructive pulmonary disease (10%), HIV/AIDS (6%), diabetes mellitus (5%), and other (7%).
The number of annual worldwide deaths the HPV vaccination can prevent:
Van Kriekinge G, Castellsague X, Cibula D, Demarteau N. Estimation of the potential overall impact of human papillomavirus vaccination on cervical cancer cases and deaths. Vaccine. 2014;32(6):733–739.
Text:
Bleich SN. A road map for sustaining healthy eating behavior. N Engl J Med. 2018;379(6):507–509.
Centers for Disease Control and Prevention. Best Practices for Comprehensive Tobacco Control Programs—2014. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.
Centers for Disease Control and Prevention. Strategies to prevent obesity and other chronic diseases: The CDC guide to strategies to increase physical activity in the community. Atlanta: U.S. Department of Health and Human Services; 2011.
Gelband H, Sankaranarayanan R, Gauvreau CL, et al. Costs, affordability, and feasibility of an essential package of cancer control interventions in low-income and middle-income countries: Key messages from Disease Control Priorities, 3rd edition. Lancet. 2016;387(10033):2133–2144.
Plummer M, de Martel C, Vignat J, Ferlay J, Bray F, Franceschi S. Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob Health. 2016;4(9):e609-616.
World Health Organization. Reducing Global Health Risks Through Mitigation of Short-Lived Climate Pollutants: Scoping Report For Policy-makers. Geneva: World Health Organization; 2015.
Wu YP, Aspinwall LG, Conn BM, Stump T, Grahmann B, Leachman SA. A systematic review of interventions to improve adherence to melanoma preventive behaviors for individuals at elevated risk. Prev Med. 2016;88:153–167.
Figure 1:
Romero Y, Trapani D, Johnson S, et al. National cancer control plans: a global analysis. Lancet Oncol. 2018;19(10):e546-e555.
Figure 2:
Thun MJ, Carter BD, Feskanich D, et al. 50-year trends in smoking-related mortality in the United States. N Engl J Med. 2013;368(4):351–64. Unpublished additional analyses.
Map 1:
Cervical Cancer Action, http://www.cervicalcanceraction.org/comments/maps.php
Figure 3:
WHO IARC Cancer Mortality Database, http://www-dep.iarc.fr/WHOdb/WHOdb.htm
Figure 4:
Adapted from Breast Health Global Initiative. Survivorship care after curative treatment for breast cancer. Available at https://www.fredhutch.org/en/labs/phs/projects/breast-cancer-initiative_2-5/knowledge-summaries/survivorship-care-survivorship-care-after-curative-treatment-for.html
Figure 5:
Global Atlas of Palliative Care at the End of Life. Available from: http://www.who.int/cancer/publications/palliative-care-atlas/en/
Explore Related Topics
This figure cannot be displayed at mobile resolutions.
To view this figure, please visit the desktop version of this website or download the PDF file of the book chapter.