Human Development Index Transitions
Understanding the transition from infection-related cancers to lifestyle-related cancers in many low- and middle-income countries is vital for planning tailored cancer control programs to reduce the future deaths and suffering from the disease.
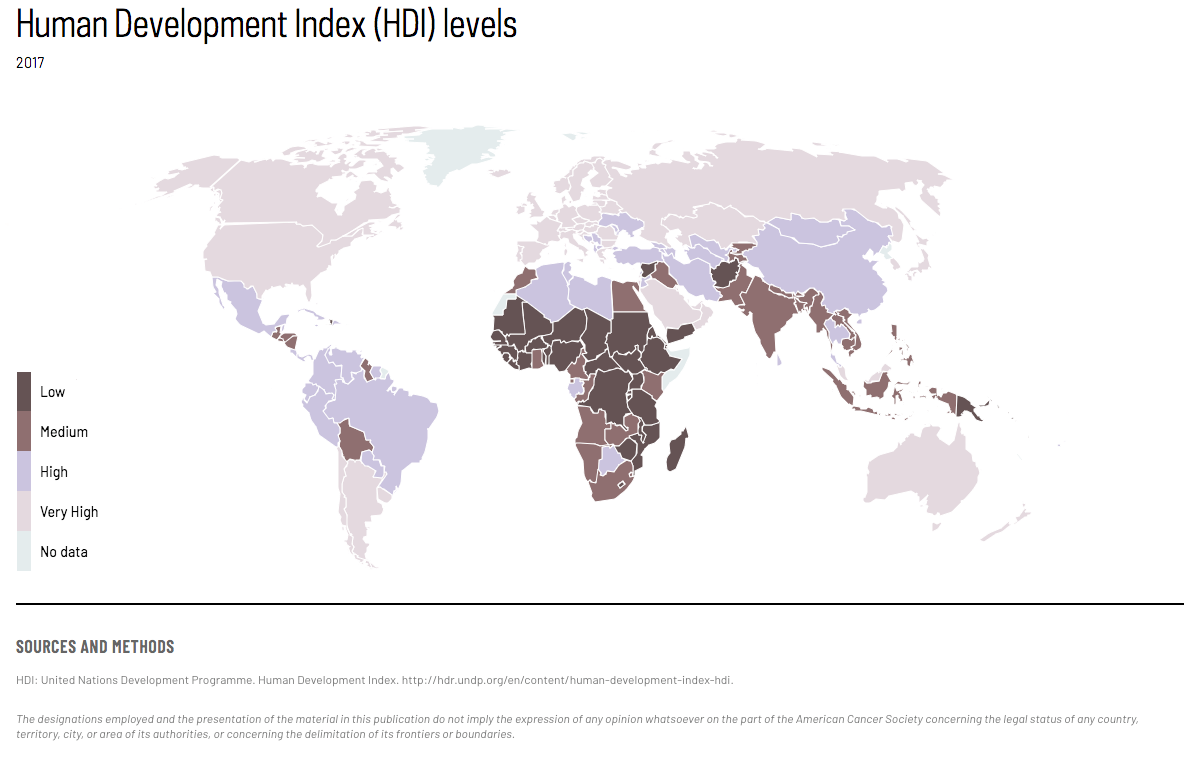
Over the last century, reductions in mortality from infectious disease, childhood and maternal conditions, and changes in fertility have led to rapid population growth and aging, and consequently an increasing burden of noncommunicable diseases, including cancer. The unsurpassed scale of the cancer problem worldwide continues to evolve as countries undergo major transitions, as measured by human development index (HDI). (Map & Figure 1)
{kind=link}
Economic growth without investment in human development is unsustainable—and unethical.
Figure 1. HDI and the top five cancers in males and females, cases in thousands, 2018. In 2018 in Very High HDI countries, there were 912 thousand Breast cancer cases in females; 491 thousand Colorectum cancer cases in males and 408 thousand in females; 545 thousand Lung cancer cases in males and 339 thousand in females; 802 thousand Prostate cancer cases in males; and 257 thousand Bladder cancer cases in males and 74 thousand in females. In 2018 in High HDI countries, there were 659 thousand Lung cancer cases in males and 315 thousand in females; 415 thousand Colorectum cancer cases in males and 323 thousand in females; 667 thousand Breast cancer cases in females; 387 thousand Stomach cancer cases in males and 181 thousand in females; and 339 thousand Liver cancer cases in males and 130 thousand in females. In 2018 in Medium HDI countries, there were 403 thousand Breast cancer cases in females; 155 thousand Lung cancer cases in males and 64 thousand in females; 206 thousand Cervix uteri cancer cases in females; 102 thousand Colorectum cancer cases in males and 72 thousand in females; and 126 thousand Lip, oral cavity cancer cases in males and 46 thousand in females. In 2018 in Low HDI countries, there were 106 thousand Breast cancer cases in females; 90 thousand Cervix uteri cancer cases in females; 54 thousand Prostate cancer cases in males; 18 thousand Colorectum cancer cases in males and 20 thousand in females; and 21 thousand Liver cancer cases in males and 12 thousand in females.
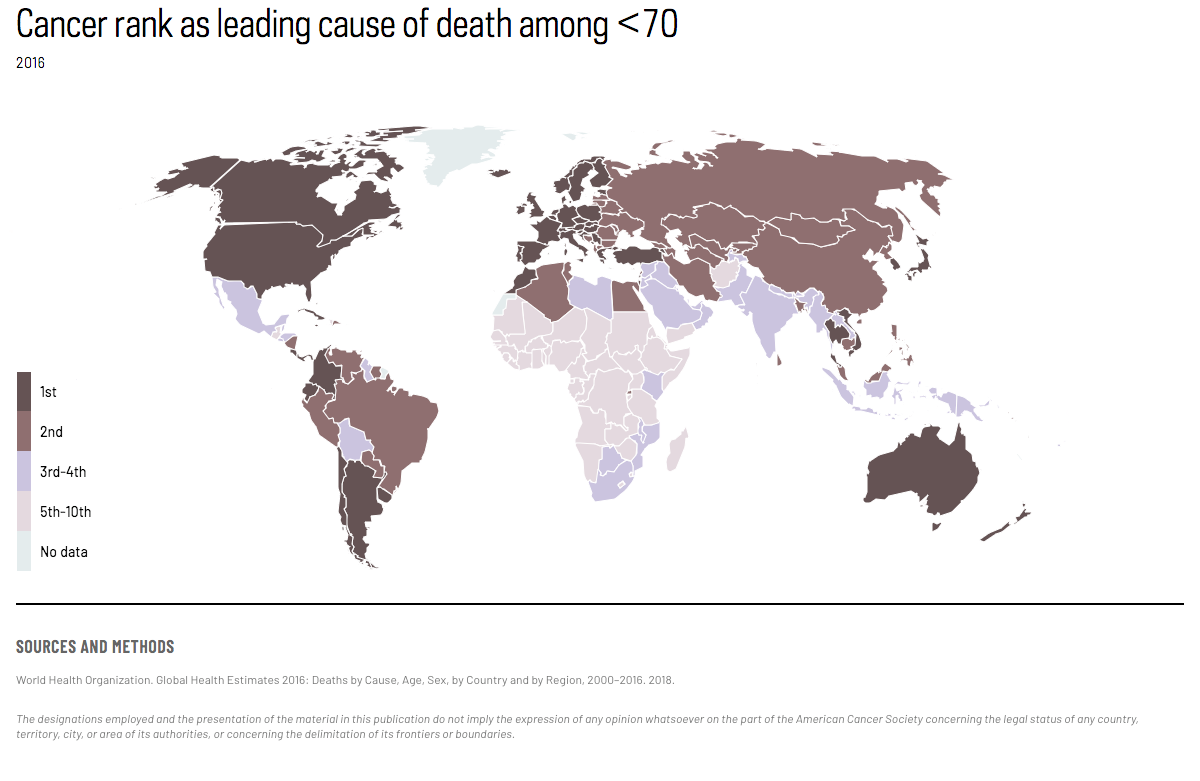
Cancer is a major cause of premature death (at ages <70) linked to socioeconomic transitions. (Map 2) It is the leading cause of premature death in 48 (predominantly very high-HDI) countries, where cancer has surpassed the first position from cardiovascular disease. In Japan, cancer now represents 45% of all premature deaths, compared with 21% due to cardiovascular disease. (Figure 2) In a further 43 countries, cancer is the second leading cause of premature death following cardiovascular disease, while both diseases rank lower in most low- and medium-HDI countries. In South Africa, for example, infectious and parasitic diseases account for 45% of premature deaths, while cancer and cardiovascular disease each account for only 10%.
{kind=link}
Figure 2. Leading causes of premature mortality (%) (ages <70 years) in South Africa and Japan. In South Africa, the leading causes of premature mortality among those less than 70 years of age are infectious and parasitic diseases (45%), cardiovascular diseases (10%), malignant neoplasms (10%), respiratory infectious diseases (6%), and other causes (24%). In Japan, the leading causes of premature mortality among those less than 70 years of age are malignant neoplasms (45%), cardiovascular diseases (21%), intentional injuries (8%), digestive diseases (5%), unintentional injuries (5%), and other causes (17%).
The profiles of cancer substantially vary by HDI, reflecting differences in lifestyle factors, entrenchment of tobacco marketing, the built environment, and the availability of detection and diagnostic services that are associated with social and economic development. Among the top 5 most commonly diagnosed cancers and 5 leading causes of cancer death by HDI, and separately for India and China, there are 16 different cancer types that rank within the top five even within these six broad “regions.” (Figure 3a & b)
The rising cancer burden will hit the lower HDI countries the hardest. Low- and medium-HDI countries, many of which are ill-equipped to deal with the present situation, are projected to have the greatest percentage increase in the burden of cancer in the coming decades. (Figure 4)
Figure 3a. In low HDI countries, the most commonly diagnosed cancers among males are prostate (20.5%); colorectum (7%); liver (8%); non-Hodgkin lymphoma (6.4%); and Kaposi sarcoma (6.3%). Other sites make up the remaining 51.7% of cancer cases. In medium HDI countries, the most commonly diagnosed cancers among males are lung (13.6%); prostate (8.8%); colorectum (8.3%); liver (10.6%); and stomach (5.3%). Other sites make up the remaining 53.4% of cancer cases. In high HDI countries, the most commonly diagnosed cancers among males are lung (13.2%); prostate (21.2%); colorectum (10.4%); stomach (6.3%); and bladder (4.9%). Other sites make up the remaining 43.9% of cancer cases. In very high HDI countries, the most commonly diagnosed cancers among males are lung (14.4%); prostate (21.2%); colorectum (13%); stomach (5.4%); and bladder (6.8%). Other sites make up the remaining 39.3% of cancer cases. In China, the most commonly diagnosed cancers among males are lung (22%); colorectum (12.9%); liver (12.4%); stomach (13.6%); and esophagus (9.1%). Other sites make up the remaining 30% of cancer cases. In India, the most commonly diagnosed cancers among males are lung (8.6%); colorectum (6.5%); stomach (6.9%); esophagus (6%); and lip and oral cavity (16.3%). Other sites make up the remaining 55.7% of cancer cases. In low HDI countries, the most common causes of cancer death among males are prostate (16.2%); colorectum (7.1%); liver (10.8%); stomach (6.1%); and non-Hodgkin lymphoma (6.7%). Other sites make up the remaining 53.1% of cancer deaths. In medium HDI countries, the most common causes of cancer death among males are lung (17.3%); colorectum (6.7%); liver (14.4%); stomach (6.3%); and esophagus (5.8%). Other sites make up the remaining 49.6% of cancer deaths. In high HDI countries, the most common causes of cancer death among males are lung (20.7%); prostate (10.9%); colorectum (9.3%); liver (7.2%); and stomach (8.7%). Other sites make up the remaining 43.3% of cancer deaths. In very high HDI countries, the most common causes of cancer death among males are lung (24.4%); prostate (9%); colorectum (11.5%); liver (6.3%); and pancreas (6.5%). Other sites make up the remaining 42.3% of cancer deaths. In China, the most common causes of cancer death among males are lung (26.4%); colorectum (8%); liver (15.3%); stomach (15.2%); and esophagus (11.1%). Other sites make up the remaining 24% of cancer deaths. In India, the most common causes of cancer death among males are lung (11.1%); colorectum (7%); stomach (8.6%); esophagus (7.6%); and lip and oral cavity (12.4%). Other sites make up the remaining 53.4% of cancer deaths.
Figure 3b. In low HDI countries, the most commonly diagnosed cancers among females are breast (26.8%); cervix (22.8%); colorectum (5%); ovary (3.7%); and non-Hodgkin lymphoma (3.1%). Other sites make up the remaining 38.6% of cancer cases. In medium HDI countries, the most commonly diagnosed cancers among females are breast (27.8%); cervix (12.6%); colorectum (6.1%); lung (5.2%); and ovary (4.8%). Other sites make up the remaining 43.5% of cancer cases. In high HDI countries, the most commonly diagnosed cancers among females are breast (27.7%); cervix (6.9%); colorectum (9.8%); lung (5.5%); and thyroid (6.2%). Other sites make up the remaining 44% of cancer cases. In very high HDI countries, the most commonly diagnosed cancers among females are breast (27%); colorectum (12%); lung (10%); thyroid (5%); and corpus uteri (6%). Other sites make up the remaining 40% of cancer cases. In China, the most commonly diagnosed cancers among females are breast (19.3%); colorectum (11.4%); lung (13.4%); thyroid (7.7%); and stomach (7.2%). Other sites make up the remaining 41% of cancer cases. In India, the most commonly diagnosed cancers among females are breast (27.9%); cervix (16.6%); colorectum (3.4%); ovary (6.2%); and lip and oral cavity (4.8%). Other sites make up the remaining 41% of cancer cases. In low HDI countries, the most common causes of cancer death among females are breast (20%); cervix (24.8%); colorectum (5.2%); ovary (4.4%); and liver (4.5%). Other sites make up the remaining 41.1% of cancer deaths. In medium HDI countries, the most common causes of cancer death among females are breast (19.3%); cervix (12.5%); colorectum (6.2%); lung (8.1%); and liver (6.4%). Other sites make up the remaining 47.6% of cancer deaths. In high HDI countries, the most common causes of cancer death among females are breast (16.7%); cervix (7.3%); colorectum (10.5%); lung (10.1%); and stomach (6.8%). Other sites make up the remaining 48.6% of cancer deaths. In very high HDI countries, the most common causes of cancer death among females are breast (14.5%); colorectum (12.5%); lung (17%); ovary (4.7%); and pancreas (7.9%). Other sites make up the remaining 43.5% of cancer deaths. In China, the most common causes of cancer death among females are breast (9.2%); colorectum (9.8%); lung (20.4%); stomach (11.1%); and liver (9%). Other sites make up the remaining 40.4% of cancer deaths. In India, the most common causes of cancer death among females are breast (23.6%); cervix (16.3%); lung (4.9%); ovary (6.5%); and lip and oral cavity (5.9%). Other sites make up the remaining 42.9% of cancer deaths.
Figure 4. Estimated millions of new cancer cases in 2018 and the projected increase by 2040 by four-tier HDI level, assuming only a demographic effect. Estimated cancer cases will increase by 100% from 2018 to 2040 in low-HDI countries, from 0.7 to 1.4 million. Estimated cancer cases will increase by 75% from 2018 to 2040 in medium-HDI countries, from 2.8 to 4.9 million. Estimated cancer cases will increase by 62% from 2018 to 2040 in high-HDI countries, from 6.5 to 10.5 million. Estimated cancer cases will increase by 32% from 2018 to 2040 in very high-HDI countries, from 8.1 to 10.7 million.
Cancer burden in 2040:
Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: IARC. Available from: https://gco.iarc.fr/today
Text:
Bray F, Jemal A, Grey N, Ferlay J, Forman D. Global cancer transitions according to the Human Development Index (2008–2030): a population-based study. Lancet Oncol. 2012;13,790-801.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Gersten O, Wilmoth JR. The cancer transition in Japan since 1951. Demographic Research. 2002;7:271–306.
Omran AR. The epidemiologic transition: A theory of the epidemiology of population change. Milbank Mem Fund Q. 1971; 49: 509–538.
United Nations Development Programme. Human Development Report 2015. Geneva: United Nations; 2015. 1–10. Available at: http://hdr.undp.org/sites/default/files/2015_human_development_report.pdf.
Map 1 and Figure 1:
HDI: United Nations Development Programme. Human Development Index. http://hdr.undp.org/en/content/human-development-index-hdi.
Cancer rates: Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: IARC. Available from: https://gco.iarc.fr/today
Map 2 and Figure 2:
World Health Organization Global Health Observatory Data Repository, http://apps.who.int/gho/data/node.home.
Figures 3 and 4:
Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: IARC. Available from: https://gco.iarc.fr/today