Sub-Saharan Africa
Up to 50% of the cancers diagnosed in some countries in Eastern Africa are still related to infection, and these are largely preventable.
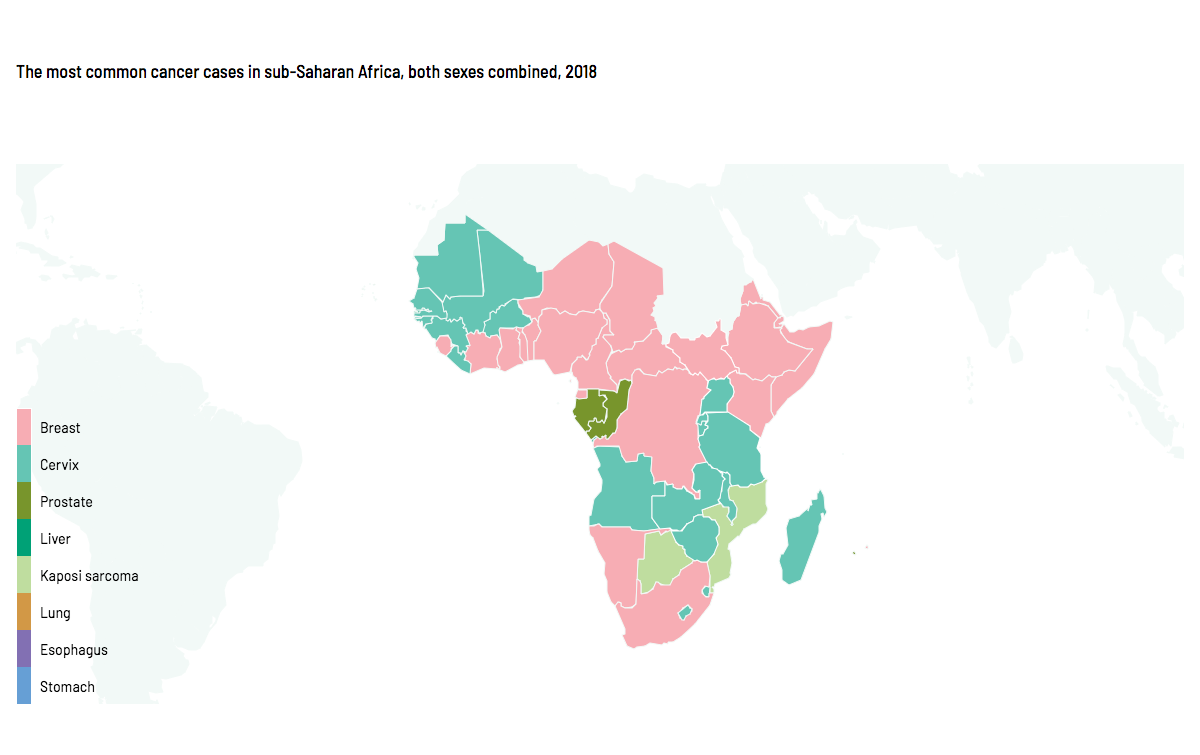
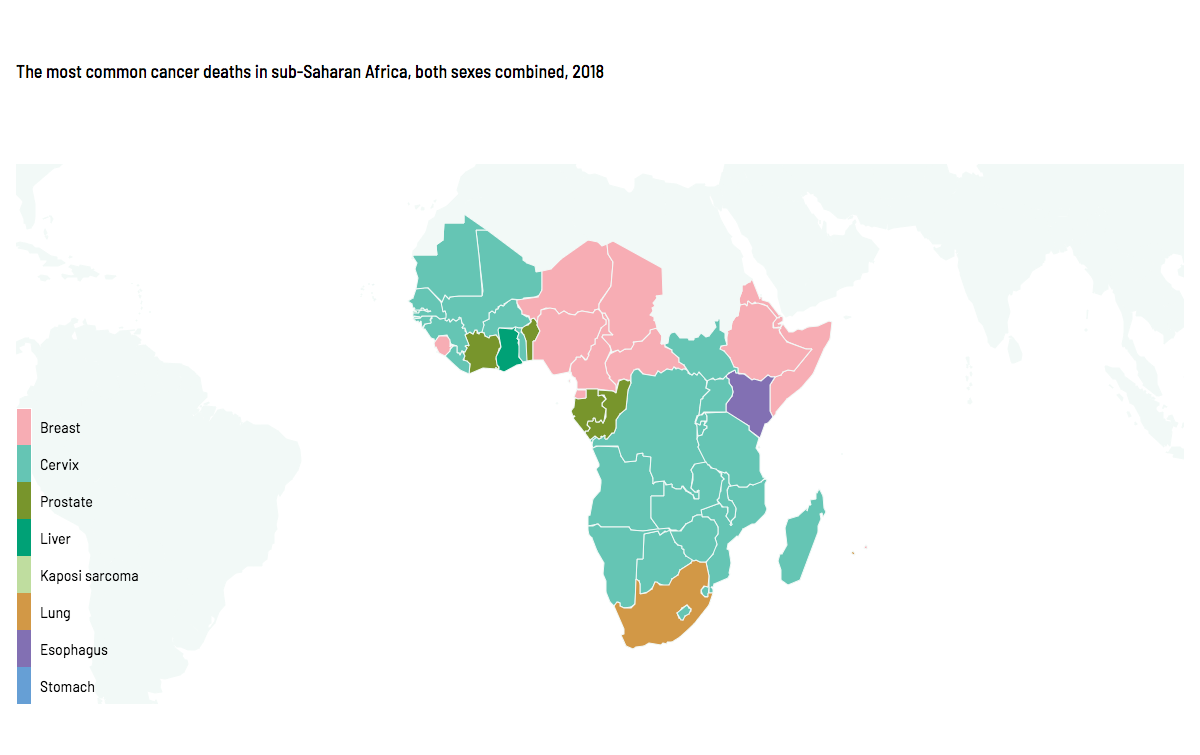
An estimated 752,000 new cancer cases (4% of the global total) and 506,000 cancer deaths occurred in sub-Saharan Africa in 2018. Although the overall cancer burden in the region is dominated by breast, cervical, and prostate cancers, the cancer profile in sub-Saharan Africa is quite diverse. (Map 1)
{kind=link}
{kind=link}
The most common cancers in men are prostate (69,000 cases, or 23% of all cancers) and liver cancers (24,000 cases, or 8% of all cancers) as well as Kaposi sarcoma (20,000 cancers, 7%). Breast (115,000 cases, 25% of all cancers) and cervical cancers (112,000 cases, 24%) are the most frequently diagnosed cancers in women. (Figure 1, 2a & b)
Figure 1. Estimated number of new cancer cases vs. deaths and distribution (%) by type (excludes non-melanoma skin cancer) in sub-Saharan Africa, both sexes, 2018. There were an estimated 752,000 cancer cases. The leading cancer cases are breast (15%), cervix (15%), prostate (9%), colorectum (6%), liver (5%), non-Hodgkin lymphoma (4%), Kaposi sarcoma (4%), and other cancers (42%). There were an estimated 506,000 cancer deaths. The leading cancer deaths are cervix (15%), breast (11%), prostate (7%), liver (7%), colorectum (6%), esophagus (5%), non-Hodgkin lymphoma (4%), and other cancers (45%).
Among males: Prostate cancer incidence 32.3, mortality 18.4. Liver cancer incidence 8.5, mortality 8.5. Colorectum cancer incidence 8.3, mortality 6. Esophagus cancer incidence 5.8, mortality 5.7. Lung cancer incidence 5.2, mortality 5.1. Non-Hodgkin lymphoma incidence 5.1, mortality 4.3. Kaposi sarcoma incidence 5.1, mortality 2.7. Stomach cancer incidence 4.9, mortality 4.7. Leukemia incidence 3, mortality 2.7. Bladder cancer incidence 2.8, mortality 1.8.
Among females: Cervix cancer incidence 34.5, mortality 25.2. Breast cancer incidence 34.2, mortality 16.6. Colorectum cancer incidence 7.5, mortality 5.1. Ovary cancer incidence 4.8, mortality 4. Liver cancer incidence 4.3, mortality 4.2. Esophagus cancer incidence 3.9, mortality 3.9. Stomach cancer incidence 3.8, mortality 3.6. Non-Hodgkin lymphoma incidence 3.7, mortality 2.4. Uterus cancer incidence 3.2, mortality 1.8. Lung cancer incidence 2.7, mortality 2.5.
Incidence rates have been increasing for several major cancer sites. For example, cervical cancer rates increased by 80% in Zimbabwe and 36% in South Africa, although they have risen and declined recently in Uganda. (Figure 3)
Major increases have been seen for breast as well as for prostate cancers where they have been measured, doubling in Zimbabwe (breast) and South Africa (both cancers) over the last 15 years. While the cause of elevated rates for certain cancers such as esophagus is still largely unknown, a westernization of lifestyle (e.g. dietary habits, fertility, excess body weight, and physical inactivity) has been related to observed increases in breast cancer, and is expected to give rise to increases in rates of other cancers such as colorectum. An improved awareness and increased capacity to perform prostatectomies on older men has been suggested to be linked to the increase in prostate cancer rates.Opportunities for reducing suffering and death from cancer in Africa exist across all stages of the cancer control spectrum.
There is a large opportunity for cancer prevention and control programs to improve health outcomes in the region. Comparing incidence and mortality rates of all cancers combined across countries, large disparities in terms of incidence-to-mortality ratios are apparent. (Figure 4) Large differences between incidence and mortality suggest poor outcomes and substantial case-fatality from cancers. Yet primary prevention remains key in sub-Saharan Africa, where there is a need to prioritize the most cost-effective means of reducing the cancer burden. Improved access to diagnosis and treatment, including palliative care, is also essential to improve survival and limit suffering from the disease in the region.
Figure 4. Incidence and mortality rates for all cancer sites combined in selected countries in sub-Saharan Africa, 2018. Age-standardized rate (world), 2018. In France, La Réunion, incidence 213.9 and mortality 95.7. In South Africa, incidence 213.5 and mortality 117. In Zimbabwe, incidence 197.5 and mortality 146.7. In Kenya, incidence 175.5 and mortality 129.2. In Malawi, incidence 166.3 and mortality 123.7. In Mauritius, incidence 153.2 and mortality 69.7. In Uganda, incidence 151.4 and mortality 110.5. In Cabo Verde, incidence 149 and mortality 111.1. In Burundi, incidence 141.9 and mortality 117.5. In Rwanda, incidence 136.4 and mortality 104.8.
Global cervical cancer deaths in sub-Saharan Africa:
Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: IARC. Available from: https://gco.iarc.fr/today.
Text:
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68(6): 394–424.
Chokunonga E, Borok MZ, Chirenje ZM, Nyakabauc AM, Parkin DM. Trends in the incidence of cancer in the black population of Harare, Zimbabwe 1991–2010. Int J Cancer. 2013; 133(3):721–9.
Jemal A, Bray F, Forman D, et al. Cancer burden in Africa and opportunities for prevention. Cancer. 2012; 118(18): 4372-84.
Somdyala NI, Parkin DM, Sithole N, Bradshaw D. Trends in cancer incidence in rural Eastern Cape Province; South Africa, 1998-2012. Int J Cancer. 2015; 136(5): E470-4.
Wabinga HR, Nambooze S, Amulen PM, Okello C, Mbus L, Parkin DM. Trends in the incidence of cancer in Kampala, Uganda 1991-2010. Int J Cancer. 2014; 135(2): 432-9.
Map and Figures 1, 2 and 4:
Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: IARC. Available from: https://gco.iarc.fr/today.
Figure 3:
Bray F, Colombet M, Mery L, et al., eds. Cancer Incidence in Five Continents, Vol. XI. Lyon: IARC. Available from: http://ci5.iarc.fr.
Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, Boyle P, eds. Cancer Incidence in Five Continents, Vol. IX. IARC Scientific Publications, No. 160. Lyon, IARC; 2007.
Forman D, Bray F, Brewster DH, et al., eds. Cancer Incidence in Five Continents, Vol. X. IARC Scientific Publication No. 164. Lyon: IARC; 2014.
Explore Related Topics
This figure cannot be displayed at mobile resolutions.
To view this figure, please visit the desktop version of this website or download the PDF file of the book chapter.