Overview of Risk Factors
Many of the known risk factors for cancer can be prevented.
Tobacco use, infectious agents, unhealthy diet, excess body weight, physical inactivity, and alcohol consumption account for the majority of cancer deaths caused by known risk factors.
Smoking causes multiple cancer types (see Risks of Tobacco), and smokeless tobacco causes cancers of the oral cavity, esophagus, and pancreas. In 2017, smoking was responsible for an estimated 2.3 million cancer deaths globally (24% of all cancer deaths), with an additional 190,000 cancer deaths due to smokeless tobacco and secondhand smoke.
Infectious agents can cause a wide range of cancer types. (Figure 1)
However, there is large variation across countries in the proportion of cancers caused by infectious agents, ranging from around 4% in many very high-income countries to more than 50% in several sub-Saharan African countries. As such, in many low-income countries infection-related cancers are a leading cause of cancer deaths (see Infection). (Figure 2)
Figure 2. Prevalence (%) of human papillomavirus (HPV) infection (all ages) and HPV vaccination (ages 10-20 years) among females by continent. In Africa, HPV vaccination prevalence is 1% and HPV prevalence is 21%. In Asia, HPV vaccination prevalence is 11% and HPV prevalence is 11%. In Latin America and the Caribbean, HPV vaccination prevalence is 19% and HPV prevalence is 17%. In Europe, HPV vaccination prevalence is 31% and HPV prevalence is 10%. In Northern America, HPV vaccination prevalence is 36% and HPV prevalence is 5%.
12 Ways to Reduce Your Risk
- Do not smoke or use any form of tobacco.
- Make your home smoke free. Support smoke-free policies in your workplace.
- Take action to be a healthy body weight.
- Be physically active. Limit the time you spend sitting.
- Have a healthy diet:
- Eat plenty of whole grains, pulses, vegetables and fruits.
- Limit foods high in sugar or fat (high-calorie) and avoid sugary drinks.
- Avoid processed meat; limit red meat and foods high in salt.
- Limit alcohol consumption. Not drinking is better for cancer prevention.
- Avoid too much sun. Use sun protection. Do not use sunbeds.
- In the workplace, follow health and safety instructions to protect yourself from harmful substances.
- Know if you are exposed to radiation from naturally high radon levels in your home. Take action to reduce high radon levels.
- For women: if you can, breastfeed your baby; limit use of hormone replacement therapy.
- Ensure your children take part in vaccination programs for hepatitis B virus and human papillomavirus.
- Take part in organized cancer screening programs for cancers of the bowel, female breast, and cervix.
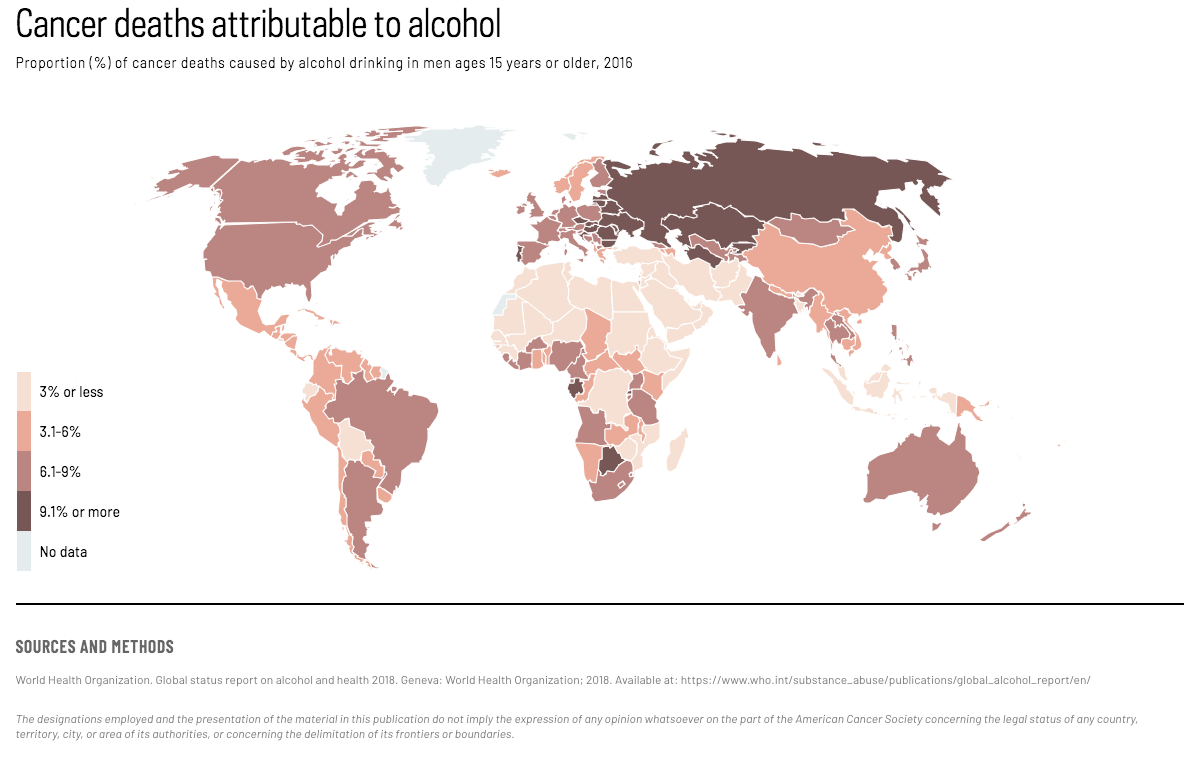
Unhealthy diet, excess body weight, and physical inactivity cause multiple types of cancer (see Body Weight, Physical Activity, Diet and Alcohol) and are emerging risk factors for cancer worldwide. The cancer burden associated with these risk factors is expected to grow in most parts of the world, particularly in parts of the Middle East and several other low- and middle-income countries in parts of Asia and Oceania because of the obesity epidemic. Further, alcohol drinking is responsible for 4.2% of all cancer deaths globally, with marked variation across countries. (Map 1)
{kind=link}
Other risk factors known to cause cancer include excessive exposure to ultraviolet radiation from the sun and indoor tanning, which cause skin cancer (see Ultraviolet Radiation); some reproductive and hormonal factors (see Reproductive and Hormonal Factors); and occupational exposures to hazardous substances and environmental pollutants such as air pollution, arsenic, and aflatoxin. (Figure 3, 4) (see Environmental and Occupational Exposures) The risk factors for cancer, however, are not limited to the above; for example, medical radiation and radiation from naturally-occurring high radon levels in residential places can cause cancer.
ACCESS CREATES PROGRESS
An inexpensive intervention to improve storage of groundnuts among subsistence farmers in Guinea reduced aflatoxin exposure by more than 50%.
Figure 3. Distribution (%) of global aflatoxin-related liver cancer by WHO region. In Africa, 40% of liver cancers are related to aflatoxin. In South-East Asia, 27% of liver cancers are related to aflatoxin. In Western Pacific, 20% of liver cancers are related to aflatoxin. In Eastern Mediterranean, 10% of liver cancers are related to aflatoxin. In Americas, 3% of liver cancers are related to aflatoxin. In Europe, 0% of liver cancers are related to aflatoxin.
Figure 4. Proportion (%) of lung cancers caused by select environmental and occupational factors other than tobacco use worldwide. Note: Does not include tobacco use. Some cancers may be attributable to two or more risk factors. Household air pollution is a cause of 17% of lung cancers. Ambient air pollution is a cause of 14% of lung cancers. Residential radon is a cause of 7% of lung cancers. Occupational risks are a cause of 7% of lung cancers.
Potentially modifiable risk factors:
Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1923–94.
Islami F, Chen W, Yu XQ, et al. Cancer deaths and cases attributable to lifestyle factors and infections in China, 2013. Ann Oncol. 2017;28(10):2567–2574.
Islami F, Goding Sauer A, Miller KD, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018;68(1):31–54.
Access creates progress:
Turner, PC, et al. Reduction in exposure to carcinogenic aflatoxins by postharvest intervention measures in west Africa: a community-based intervention study. Lancet. 2005;365(9475):1950–1956.
Text:
Bouvard V, Baan R, Straif K, et al. A review of human carcinogens–Part B: biological agents. Lancet Oncol. 2009;10(4):321–322.
Bruni L, Diaz M, Barrionuevo-Rosas L, et al. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. Lancet Glob Health. 2016;4(7):e453-463.
Bruni L, Diaz M, Castellsague X, Ferrer E, Bosch FX, de Sanjose S. Cervical human papillomavirus prevalence in 5 continents: meta-analysis of 1 million women with normal cytological findings. J Infect Dis. 2010;202(12):1789–1799.
El Ghissassi F, Baan R, Straif K, et al. A review of human carcinogens–part D: radiation. Lancet Oncol. 2009;10(8):751–752.
GBD Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100): 1345–1422.
GBD Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906.
Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018.
IARC Working Group. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, vol 100E: Personal Habits and Indoor Combustions. Lyon: IARC Press; 2012.
Islami F, Chen W, Yu XQ, et al. Cancer deaths and cases attributable to lifestyle factors and infections in China, 2013. Ann Oncol. 2017;28(10): 2567–2574.
Islami F, Goding Sauer A, Miller KD, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018;68(1):31–54.
Islami F, Stoklosa M, Drope J, Jemal A. Global and regional patterns of tobacco smoking and tobacco control policies. Eur Urol Focus. 2015(1):3–16.
Liu Y, Wu F. Global burden of aflatoxin-induced hepatocellular carcinoma: a risk assessment. Environ Health Perspect. 2010;118(6):818–824.
Pearson-Stuttard J, Zhou B, Kontis V, Bentham J, Gunter MJ, Ezzati M. Worldwide burden of cancer attributable to diabetes and high body-mass index: a comparative risk assessment. Lancet Diabetes Endocrinol. 2018;6(6):e6-e15.
Plummer M, de Martel C, Vignat J, Ferlay J, Bray F, Franceschi S. Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob Health. 2016;4(9):e609-616.
Prüss-Ustün A, Wolf J, Corvalán C, Bos R, Neira M. Preventing disease through healthy environments: a global assessment of the burden of disease from environmental risks. Switzerland, Geneva: WHO Press; 2016.
Schuz J, Espina C, Villain P, et al. European Code against Cancer 4th Edition: 12 ways to reduce your cancer risk. Cancer Epidemiol. 2015;39 Suppl 1:S1-10.
World Cancer Research Fund/American Institute for Cancer Research. Diet, nutrition, physical activity and cancer: a global perspective. Continuous Update Project Expert Report 2018. Available at dietandcancerreport.org.
Xia C, Zheng R, Zeng H, et al. Provincial-level cancer burden attributable to active and second-hand smoking in China. Tob Control. 2018.
Map:
World Health Organization. Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018. Available at: https://www.who.int/substance_abuse/publications/global_alcohol_report/en/
Figure 1:
Bouvard V, Baan R, Straif K, et al. A review of human carcinogens–Part B: biological agents. Lancet Oncol. 2009;10(4):321–322.
Plummer M, de Martel C, Vignat J, Ferlay J, Bray F, Franceschi S. Global burden of cancers attributable to infections in 2012: A synthetic analysis. Lancet Glob Health. 2016;4(9):e609-616.
Figure 2:
Bruni L, Diaz M, Castellsague X, Ferrer E, Bosch FX, de Sanjose S. Cervical human papillomavirus prevalence in 5 continents: Meta-analysis of 1 million women with normal cytological findings. J Infect Dis. 2010;202(12):1789–1799.
Bruni L, Diaz M, Barrionuevo-Rosas L, et al. Global estimates of human papillomavirus vaccination coverage by region and income level: A pooled analysis. Lancet Glob Health. 2016;4(7):e453-463.
Figure 3:
Liu Y, Wu F. Global burden of aflatoxin-induced hepatocellular carcinoma: a risk assessment. Environ Health Perspect. 2010;118(6):818–824.
Figure 4:
Prüss-Ustün A, Wolf J, Corvalán C, Bos R, Neira M. Preventing disease through healthy environments: a global assessment of the burden of disease from environmental risks. Geneva: WHO Press; 2016.
Text box:
Schuz J, Espina C, Villain P, et al. European Code against Cancer 4th Edition: 12 ways to reduce your cancer risk. Cancer Epidemiol. 2015;39 Suppl 1:S1-10.