Risks of Tobacco
Tobacco use is the leading preventable cause of cancer worldwide. Fortunately, reductions in smoking yield large reductions in cancer incidence and mortality.
An estimated 1.3 billion people use tobacco products worldwide. The majority (about 1.1 billion) use smoked tobacco products, chiefly as manufactured or hand-rolled cigarettes. Other smoked products include pipes, cigars, bidi, hookah, and/or kreteks; smokeless products include snuff, chewing tobacco, and betel. Novel tobacco products, especially recently redesigned e-cigarettes, increasingly dominate tobacco use among youth in some high-income countries (HIC). (Figure 1)
{kind=link}
{kind=link}
Figure 1. Cigarette and e-cigarette use (%) among high schoolers, United States, 2011-2018. Cigarette use among US high schoolers has decreased from 15.8% in 2011 to 8.1% in 2018. E-cigarette use among US high schoolers has increased from 1.5% in 2011 to 20.8% in 2018.
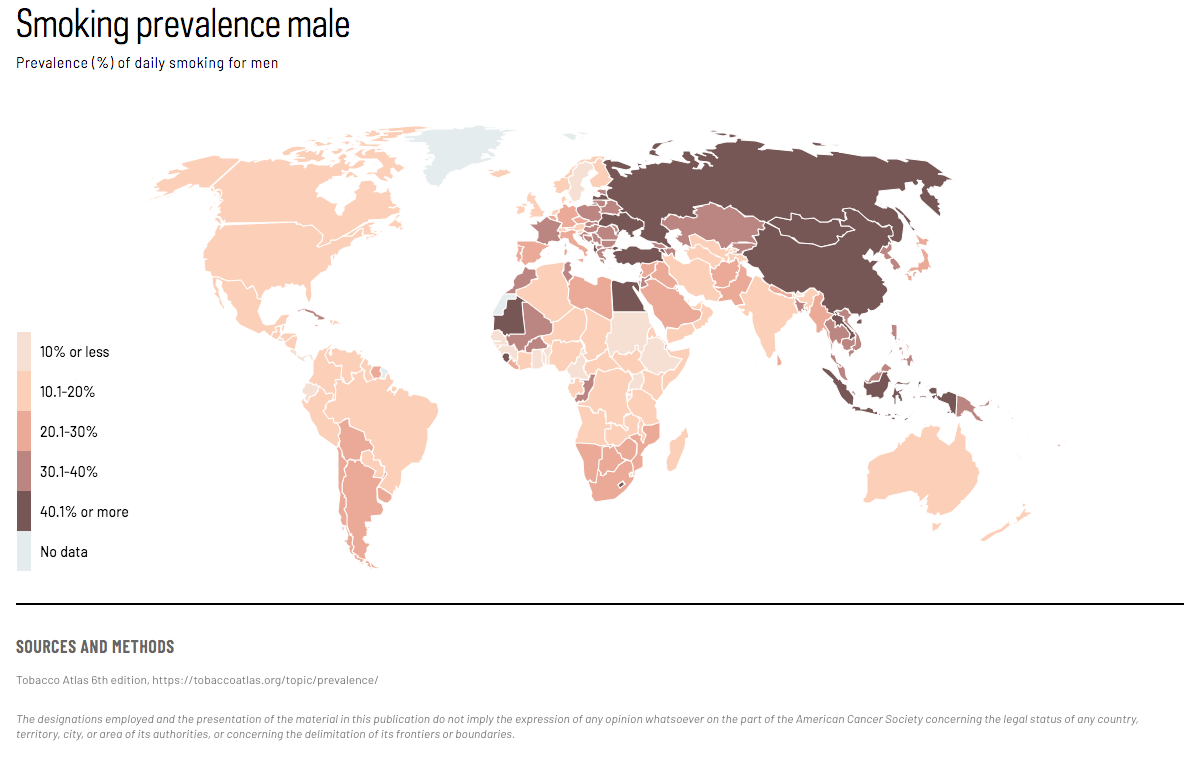
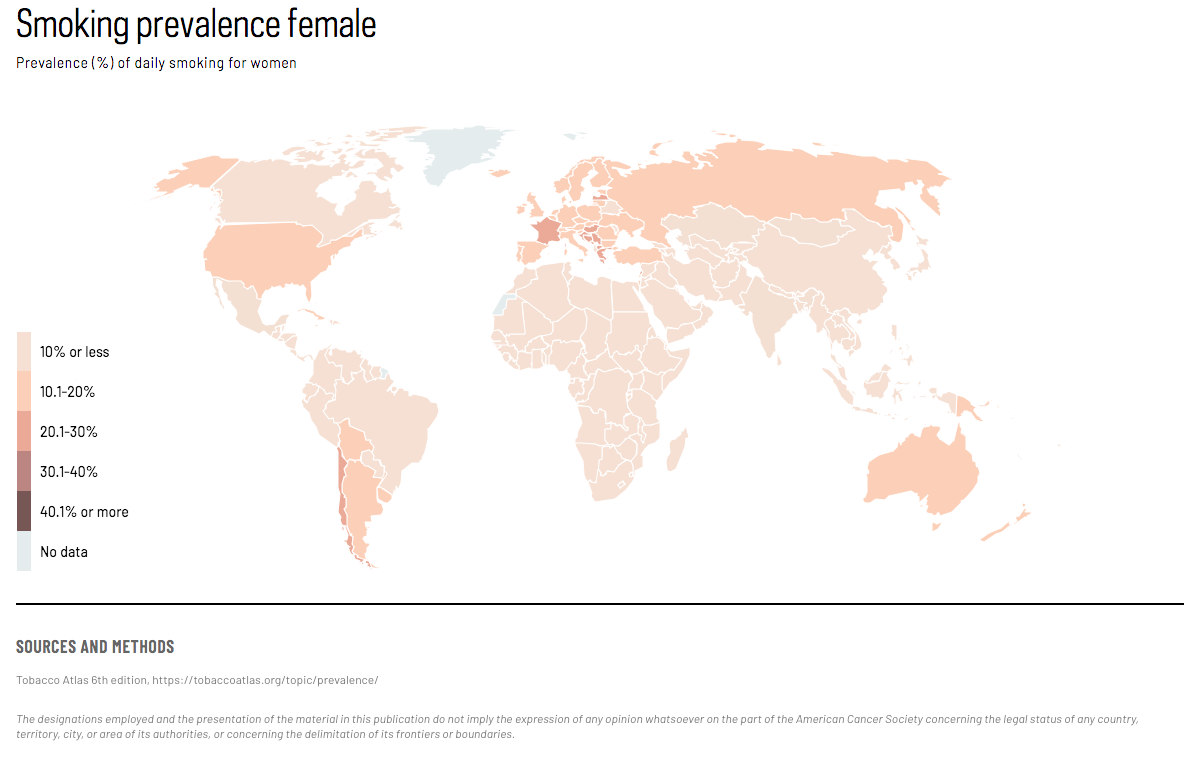
Eighty percent of the world’s smokers live in low and middle income countries (LMIC). The enormous global health and economic burden from tobacco use is increasingly borne by LMIC, due to population aging and the massive numbers of people who continue to smoke. Although smoking prevalence and per-capita consumption are decreasing worldwide, the rate of decrease is slower in LMIC than in HIC, and among women than men in HIC.
All smoked and traditional smokeless tobacco products cause cancer. Although lung cancer is the most common cancer caused by cigarette smoking, at least 19 other cancer sites or subsites are designated as causally related to smoking. (Figure 2a & b)
We know what works to reduce tobacco use and tobacco-related cancers. Our responsibility now is to implement it.
Figure 1a. Proportion (%) of annual cancer deaths attributable to smoking by site, 2010-2014, United States. 22% of cervical cancer deaths are attributable to smoking. 10% of pancreatic cancer deaths in men and 14% in women are attributable to smoking. 11% of colorectal cancer deaths in men and 8% in women are attributable to smoking. 22% of kidney and other urinary tract cancer deaths in men and 7% in women are attributable to smoking. 23% of acute myeloid leukemia deaths in men and 3% in women are attributable to smoking. 26% of stomach cancer deaths in men and 11% in women are attributable to smoking. 28% of liver cancer deaths in men and 14% in women are attributable to smoking. 47% of bladder cancer deaths in men and 41% in women are attributable to smoking. 49% of lip, oral cavity, and pharyngeal cancer deaths in men and 43% in women are attributable to smoking. 52% of esophageal cancer deaths in men and 44% in women are attributable to smoking. 72% of laryngeal cancer deaths in men and 93% in women are attributable to smoking. 83% of lung, bronchus, and trachea cancer deaths in men and 76% in women are attributable to smoking.
Figure 1b. Number of annual cancer deaths attributable to smoking by site, 2010-2014, United States. 862 cervical cancer deaths are attributable to smoking. 1,870 pancreatic cancer deaths in men and 2,626 in women are attributable to smoking. 2,976 colorectal cancer deaths in men and 1,992 in women are attributable to smoking. 1,904 kidney and other urinary tract cancer deaths in men and 350 in women are attributable to smoking. 1,181 acute myeloid leukemia deaths in men and 136 in women are attributable to smoking. 1,656 stomach cancer deaths in men and 476 in women are attributable to smoking. 4,085 liver cancer deaths in men and 975 in women are attributable to smoking. 4,920 bladder cancer deaths in men and 1,804 in women are attributable to smoking. 2,955 of lip, oral cavity, and pharyngeal cancer deaths in men and 1,077 in women are attributable to smoking. 6,011 esophageal cancer deaths in men and 1,296 in women are attributable to smoking. 2,125 laryngeal cancer deaths in men and 730 in women are attributable to smoking. 72,164 lung, bronchus, and trachea cancer deaths in men and 53,635 in women are attributable to smoking.
Even this list may be incomplete, as it does not include breast cancer or advanced prostate cancer, two sites for which the evidence has been labeled suggestive but not conclusive. Cigar and pipe smoking cause cancers of the lung and upper aerodigestive tract, including the oral cavity, oropharynx, hypopharynx, larynx and esophagus; secondhand smoke causes lung cancer. Smoked tobacco products cause even more deaths from vascular and respiratory conditions than from cancer. Cessation of smoking dramatically reduces risks compared to continued smoking.
ACCESS CREATES PROGRESS
Access to smoking cessation aids such as counseling, telephone quit lines, and pharmacotherapy can help people quit smoking. Even brief counseling encounters have been shown to increase quit rates, and a combination of counseling and pharmacotherapy can further increase success.
Male smoking prevalence:
Dr. Michael Thun, personal communication
Access creates progress:
Siu AL, for the US Preventive Services Task Force. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: USPSTF Recommendation Statement for Interventions for Tobacco Smoking Cessation. Ann Intern Med. 2015;163(8):622–634.
Text:
Asma S, Mackay J, Song SY, et al. The GATS Atlas. Atlanta, GA: CDC Foundation 2015. Available at www.gatsatlas.org.
Drope J, Schluger N, Cahn Z, et al. The Tobacco Atlas. Atlanta: American Cancer Society and Vital Strategies, 2018 Available at https://tobaccoatlas.org/topic/prevalence/.
Thun MJ, Freedman ND. Tobacco. In: Thun MJ, Linet MS, Cerhan JR, Haiman CA, Schottenfeld (Eds), Schottenfeld and Fraumeni. Cancer Epidemiology and Prevention, (4th ed., pp 185–211). New York: Oxford University Press, 2018
Gentzke AS, Creamer M, Cullen KA, et al. Vital Signs: Tobacco Product Use Among Middle and High School Students — United States, 2011–2018. MMWR Morb Mortal Wkly Rep. 2019;68:157–164.
Huang J, Duan Z, Kwok J, et al. Vaping versus JUULing: How the extraordinary growth and marketing of JUUL transformed the US retail e-cigarette market. Tobacco Control. 2019;28:146–151.
US National Cancer Institute. Patterns of tobacco use, exposure, and health consequences. In: The Economics of Tobacco and Tobacco Control, Tobacco Control Monograph 21. Bethesda, MD and Geneva: U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute and World Health Organization. 2016.
IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Volume 100: A Review of Human Carcinogens. Part E: Personal Habits and Indoor Combustions. Lyon, France: IARC,2012.
US Department of Health and Human Services. The Health Consequences of Smoking- 50 Years of Progress: A Report of the Surgeon General. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.
Map:
Tobacco Atlas 6th edition, https://tobaccoatlas.org/topic/prevalence/
Figure 1:
Gentzke AS, Creamer M, Cullen KA, et al. Vital Signs: Tobacco Product Use Among Middle and High School Students — United States, 2011–2018. MMWR Morb Mortal Wkly Rep. 2019;68:157–164.
Figure 2:
Notes: Lip cancer classified as causal in 1964, other oropharyngeal cancers in 1971. Lung cancer classified as causal in men in 1964 and in women in 1968. Esophagus, lung, and kidney include multiple histologic subtypes. Source: Modified from US Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.