Cancer Survivorship
People are living longer after a cancer diagnosis due to advances in early detection and treatment. There are close to 54 million people worldwide who are currently diagnosed with a cancer diagnosis within five years (Figure 31.1).
Estimated number of prevalent cases (5-year) by cancer type, 2022

Although most cancer survivors are currently concentrated in high-income countries (Map 31.1), the number is expected to grow faster in transitioning countries due to increasing cancer incidence, improving cancer survival, and population growth and ageing.
Individuals are considered “cancer survivors” from diagnosis and throughout their lifetime. Although this term may or may not resonate with all individuals, it is meant to encompass individuals with a history of cancer. “Cancer survivorship care” refers to efforts to enhance health and well-being during and beyond treatment, aiming to prevent and mitigate acute, long-term, and late-occurring effects of cancer, which also benefits families and informal caregivers (Figure 31.2). In addition to health-related difficulties, cancer survivors often face medical financial hardship (see Economic Burden). In the United States, approximately 60% of working-age cancer survivors report at least one type of financial hardship, such as foregoing or delaying medical care because of cost. A study from seven Southeast Asian countries found that over 75% of patients faced death or catastrophic health expenditure within a year of diagnosis.
Long-term and late-effects of cancer diagnosis and treatment
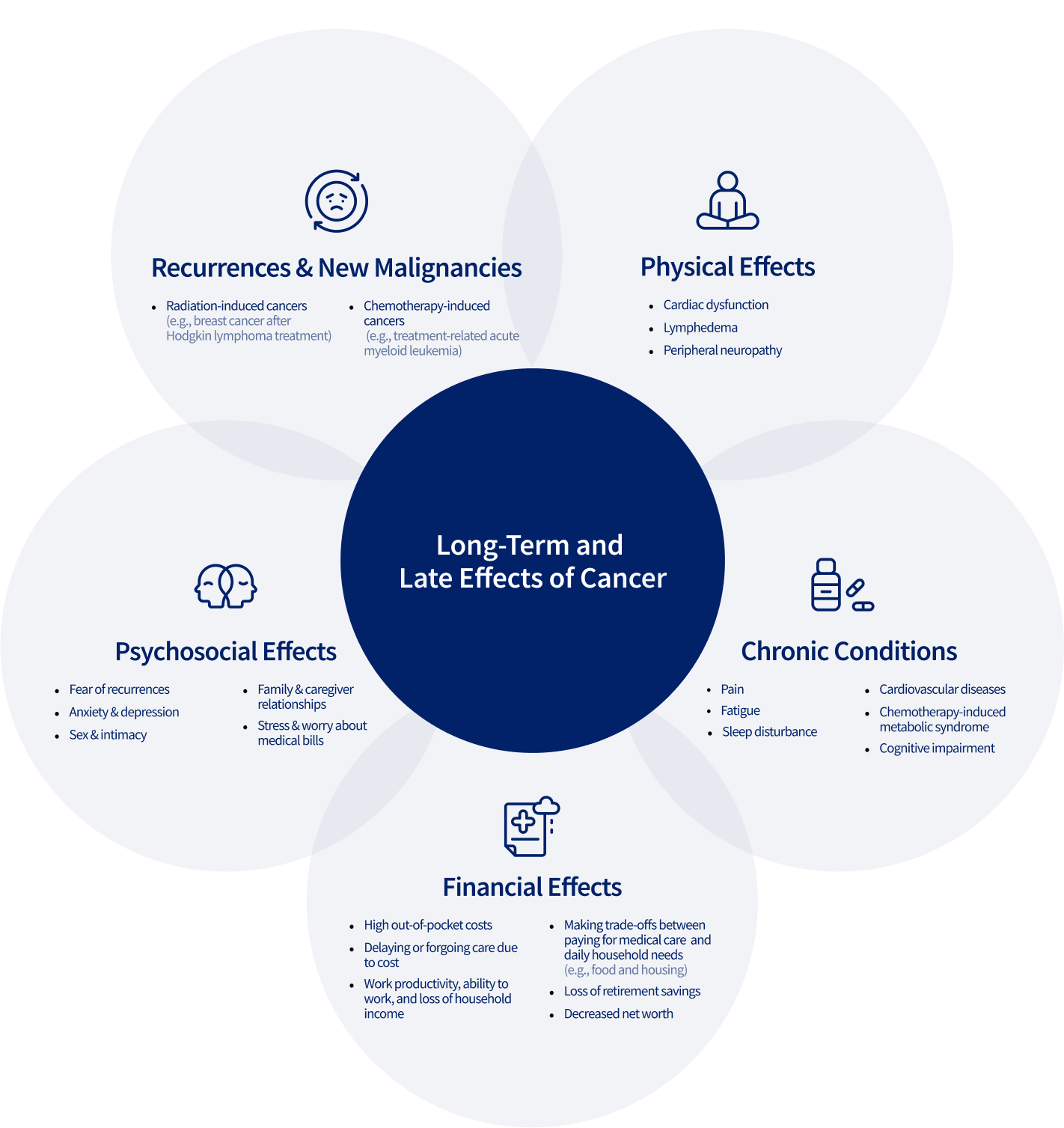
“Addressing the emotional, psychological, and social challenges of survivorship is as essential as treating the disease itself.”
Many countries are seeking to transform health care delivery to address cancer survivors’ needs. For example, the United Kingdom has implemented personalized follow-up care, triaging survivors based on individual needs, improving their quality of life and in doing, saving 110 million US dollars over five years. In countries with constrained resources, however, survivorship care is often overlooked; only 9% of low-income countries address survivorship care in their non-communicable disease plan or national cancer-control plans, compared with 66% of high-income countries (see Cancer Continuum). To advance equitable survivorship care globally, the implementation of resource-conscious guidelines in national cancer-control plans is needed, supported by more research in transitioning countries and increased collaboration and regional partnerships (Figure 31.3).
Recommendations for advancing equitable cancer survivorship care across the globe