Geographic Diversity
There are an estimated 19 million new cancer cases and 9.7 million cancer deaths (excluding non-melanoma skin cancer) worldwide each year. Over half of the cases (9.7 million) and 56% of the deaths (5.4 million) occur in Asia (Figure 22.1), where 60% of the global population (4.6 billion) reside. Europe has the second highest cancer burden, with 4 million new cases (22% of the total burden) and 2 million cancer deaths (20%), followed by North America for incidence, with 2.1 million new cases (11% of the global burden) and Africa for mortality, with 0.8 million deaths (8% of the global burden). The disproportional contribution of Europe and North America to the global cancer burden contrasts with their relatively small population sizes, which make up only 9% and 5% of the global population, respectively.
Estimated number of cases and deaths (excluding non-melanoma skin cancer) by continent, 2022
Among men, prostate cancer dominates in most countries as the most commonly diagnosed cancer, followed by lung. For mortality, this is reversed, with lung cancer being the leading cause of death followed by prostate cancer (Map 22.1).
Among women, breast cancer is the most diagnosed cancer in almost all countries globally (158 countries) and the leading cause of death in 111 countries, followed by cervical cancer in 24 countries for incidence and 38 countries for mortality, most of which are in sub-Saharan Africa (Map 22.2).
“I have a neighbor who knows 200 types of wine. … I only know two types of wine – red and white. But my neighbor only knows two types of countries – industrialized and developing. And I know 200.”
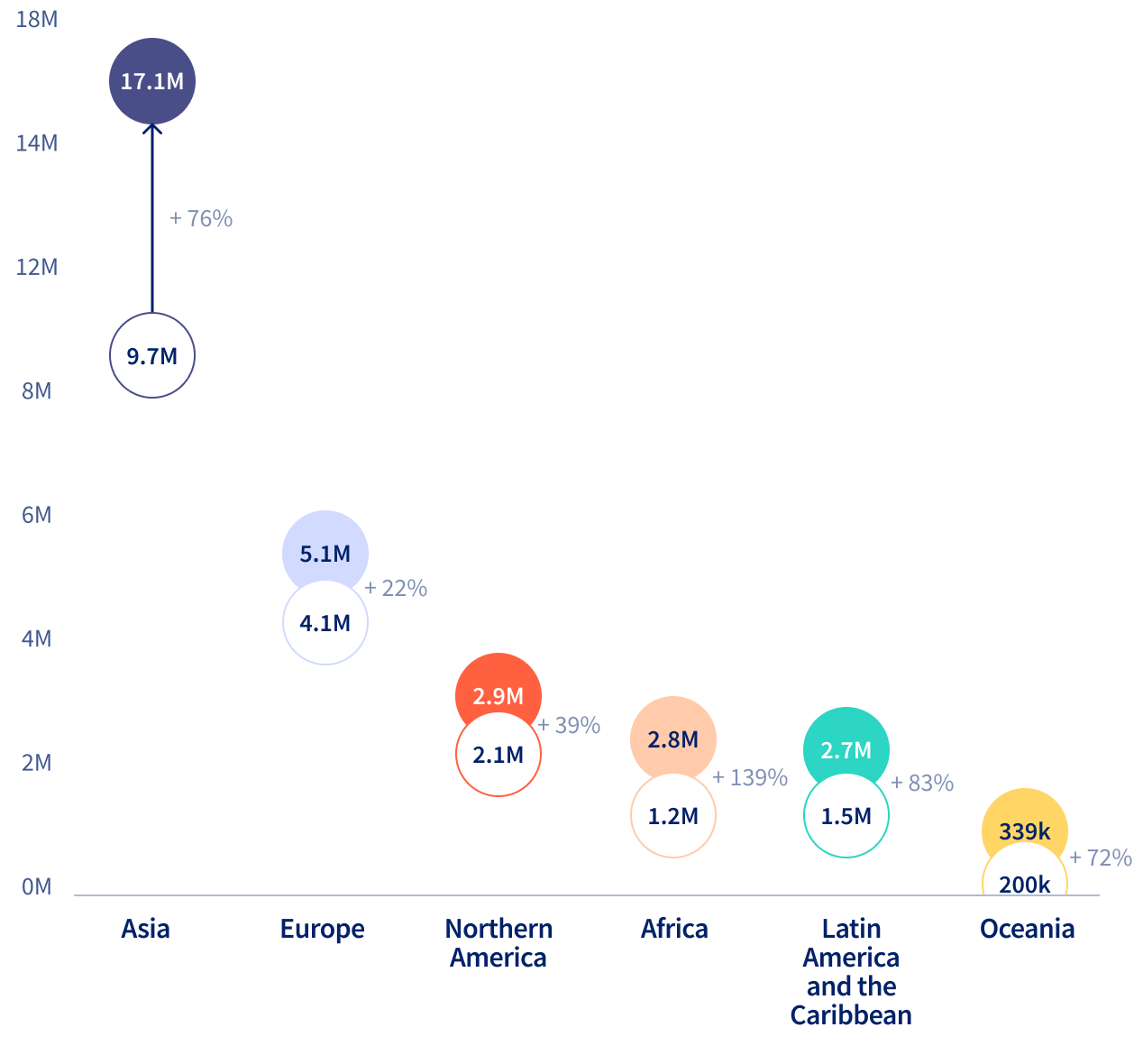
The patterns of cancer that we observe can be linked to the underlying risk factors, diagnostic practices, early detection programs, and access to and availability of treatment. Such factors are discussed in detail in each regional chapter (see Chapters 23-29). As well as population size, the age structure of the populations – and their evolution – in different global regions also differs. This demographic transition will have a major impact on the future cancer burden, e.g., the incident cases are expected to increase by 139% in Africa by 2050, compared to 22% in Europe (Figure 22.2).
Regional differences in population aging will shape future cancer burdens, with cases projected to rise 139% in Africa by 2050, compared to 22% in Europe.
Estimated number of new cases for all cancers (excluding non-melanoma skin cancers) combined from 2022 to 2050 across continents