Liver Cancer
Hepatitis B virus infection accounts for over half of all liver cancer cases occurring each year worldwide.
Liver cancer is the sixth most frequently occurring cancer in the world, but due to the poor prognosis associated with the disease, it is the third largest contributor to cancer mortality, with an estimated 870,000 cases and 760,000 deaths in 2022 (Map 18.1).
The highest incidence rates per 100,000 persons occur in Micronesia (26.4), Eastern Asia (22.4), and Southeast Asia (21.2) in men and Northern Africa (10.1) and Eastern Asia (7.2) in women (Figure 18.1). The lowest rates are in Western and South Central Asia in both men and women. In almost all regions, rates among men are two to four times higher than those among women. In Central America and the Caribbean, however, the male-to-female ratio is less than 1.5.
Liver cancer incidence, age-standardized rate (world) per 100,000, by UN region and sex, 2022

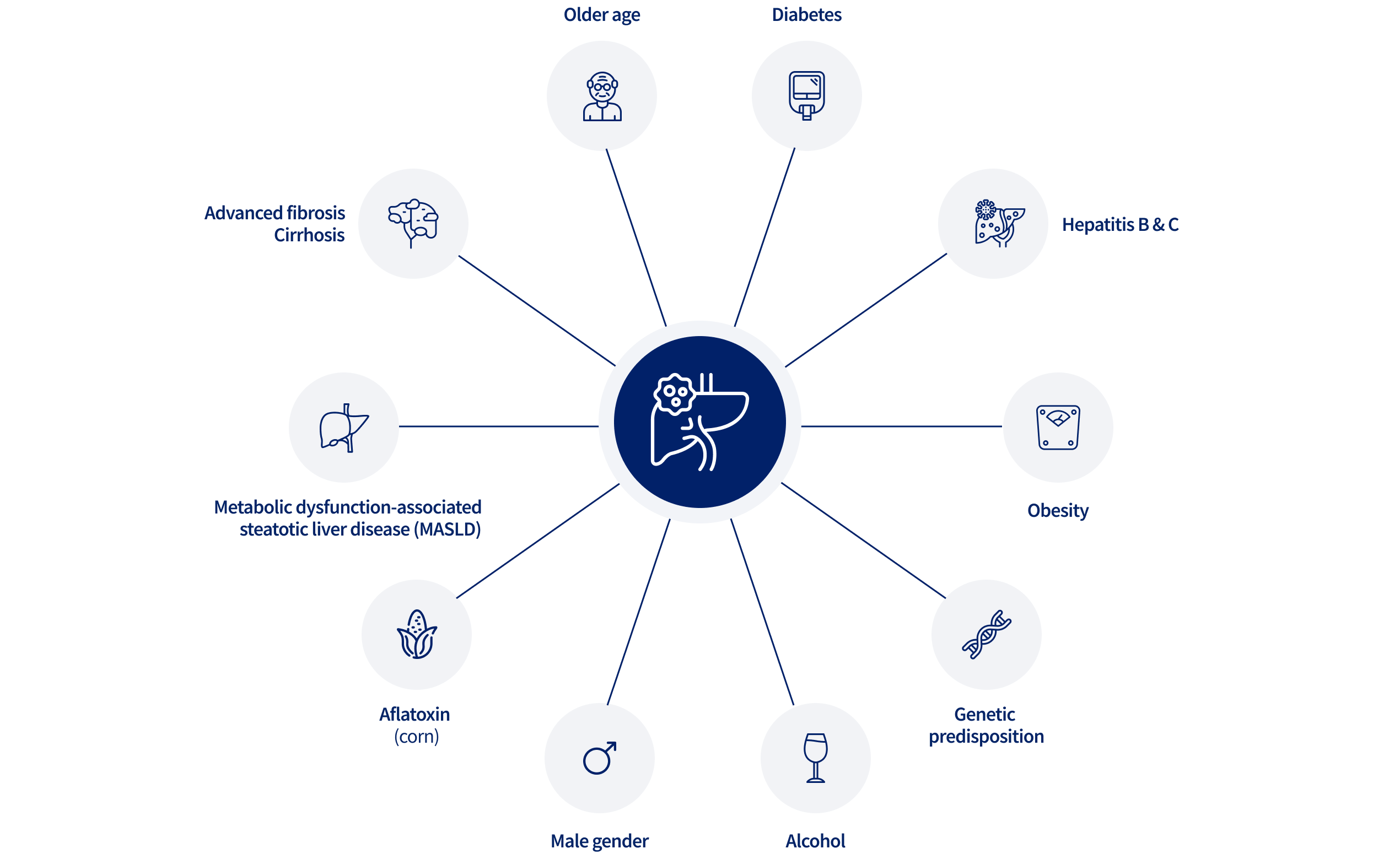
Major risk factors for liver cancer include hepatitis B virus (HBV), hepatitis C virus (HCV), aflatoxin B1 (AFB1), alcohol consumption, cigarette smoking, and the related conditions of excess body fatness, type-2 diabetes, and metabolic dysfunction-associated steatotic liver disease (MASLD) (Figure 18.2). HBV, the dominant risk factor globally, accounts for approximately 55% of liver cancers in the world, while HCV accounts for 21% of the cases (see Infection). In general, HBV and AFB1 are more common risk factors in much of Eastern Asia and sub-Saharan Africa, while HCV and alcohol are more common factors in North America and Europe.
Major risk factors of liver cancer
“By addressing the root causes and implementing effective strategies, we can prevent unnecessary suffering, premature deaths, and the economic burden caused by hepatitis and liver cancer.”
The prevalence of these risk factors has been changing, affecting liver cancer incidence in recent decades. Rates in some traditionally high-risk countries such as China, Japan, and the Republic of Korea, began to decline in the late 20th century (Figure 18.3). The decline is likely related to a reduction in AFB1 exposure, the initiation of neonatal HBV vaccination, and the advent of antiviral therapy for HCV infection. In contrast, rates in many lower-risk countries, such as the United States, the United Kingdom, and Australia, began increasing in the later decades of the 20th century (Figure 18.4). The increase is likely related to the spread of HCV in the mid-20th century, as well as the increasing prevalence of MASLD. The recent stabilization of incidence rates in some of these countries (e.g., the United States) may reflect the removal of HCV from national blood supplies. MASLD is now becoming the most common cause of liver cancer in many countries.
Liver cancer rates have declined in historically high-risk countries since the late 20th century, likely due to reduced aflatoxin exposure, HBV vaccination at birth, and improved HCV treatment.
Trends in liver cancer incidence, age-standardized rate (world) per 100,000, in selected countries, Eastern Asia, 1975-2017
In historically lower-risk countries, liver cancer rates are rising, likely due to HCV spread and rising metabolic dysfunction-associated steatotic liver disease.
Trends in liver cancer incidence, age-standardized rate (world) per 100,000, in selected high-income Western countries, 1975-2017
Liver cancer reduction strategies for HBV infection include neonatal vaccination and antiviral therapy among persons chronically infected; for HCV, they include antiviral therapy to eliminate the virus among persons chronically infected; for AFB1, they include pre- and post-harvest strategies to reduce/eliminate exposure; for alcohol and tobacco, they include reduction/cessation of exposure; and for metabolic conditions, they include maintenance of bodyweight below obesity and adherence to anti-diabetes therapy.