Cancer in Indigenous Populations
Higher prevalence of risk factors, poor outcomes, and under-reporting are among the cancer control challenges for Indigenous peoples.
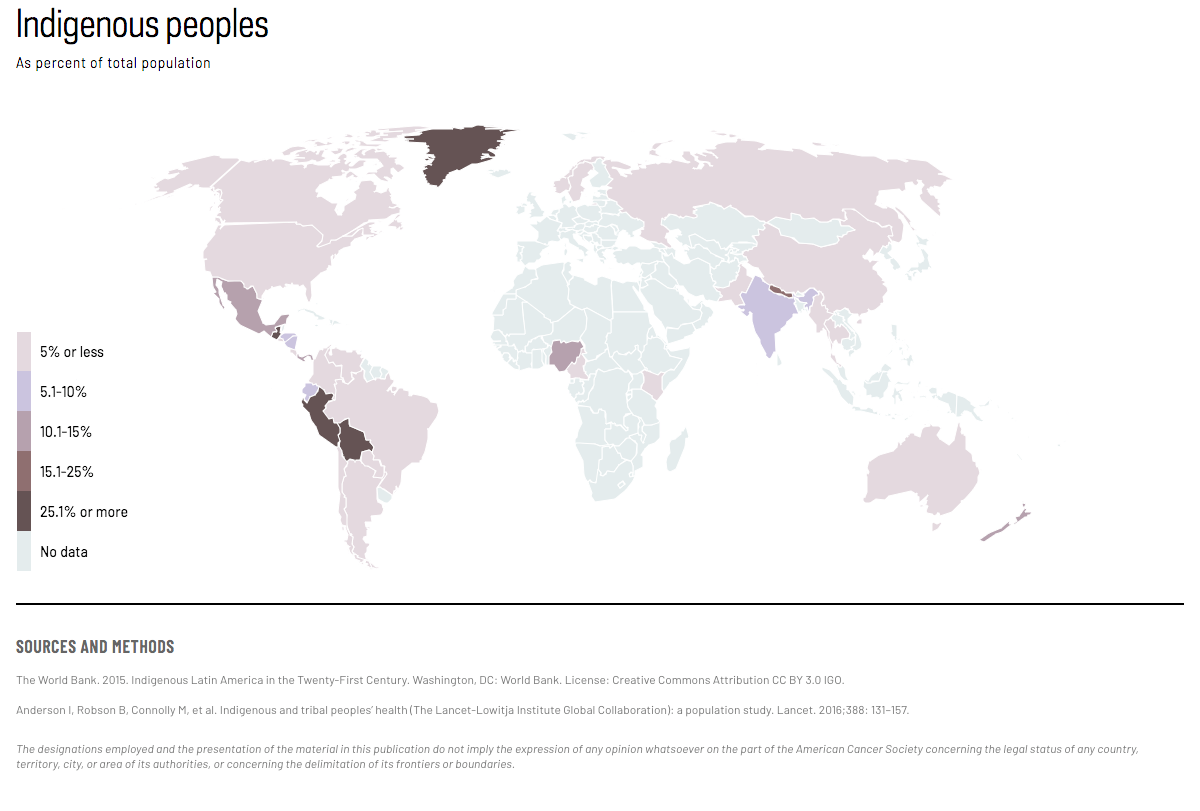
There are more than 370 million Indigenous people spanning at least 70 countries worldwide. Indigenous peoples generally face disadvantage and have worse health than non-Indigenous people. Data related to cancer in these populations tend to be absent or of poor quality making many Indigenous peoples statistically invisible, with the majority of data that exist coming from a few high-income countries.
{kind=link}
ACCESS CREATES PROGRESS
New Zealand is the only country in the world that routinely records and reports national-level cancer statistics for its Indigenous population.
Hei Ahuru Mowai, Aotearoa/ New Zealand’s Indigenous Māori cancer leadership group, aims to influence national cancer policy by ensuring participation and engagement with Māori from policy development to implementation across the cancer control continuum. The group has representatives on most of the country’s cancer groups and also partnered with the Ministry of Health on a Cancer and Racism seminar which will inform a new national cancer strategy. Hei Ahuru Mowai is currently working with the National Bowel Screening Programme to ensure equity is addressed in its national roll-out.

There is under-reporting of cancer incidence and mortality in many jurisdictions. Indigenous peoples often have higher incidence and mortality rates of cancers related to exposure to tobacco, alcohol, poor diet, physical inactivity, high BMI, and diabetes mellitus than non-Indigenous people living in the same countries, although cancer patterns vary from country to country. (Figure 1a & b)
Figure 1. Relative risk of cancer-specific mortality for Indigenous compared with non-Indigenous peoples by country and site. Source varies by country. See Sources and Methods.
Among males: In New Zealand (2006-2011), cancer death risk in Indigenous populations compared with non-Indigenous is 3.5 times higher for lung; 3.5 times higher for stomach; 18% higher for colorectum; and 2 times higher for prostate. In Alaska, United States (1999-2009), cancer death risk in Indigenous populations compared with non-Indigenous is 43% higher for lung; 4.4 times higher for stomach; 2.1 times higher for colorectum; and 7% lower for prostate. In Australia (2012-2016), cancer death risk in Indigenous populations compared with non-Indigenous is 58% higher for lung; 77% higher for stomach; 4% lower for colorectum; and 10% lower for prostate. In the United States (2012-2016), cancer death risk in Indigenous populations compared with non-Indigenous is 11% lower for lung; 2.2 times higher for stomach; 17% higher for colorectum; and 6% higher for prostate. Among Métis in Canada (1991-2001), cancer death risk in Indigenous populations compared with non-Indigenous is 21% higher for lung; 18% lower for stomach; 27% lower for colorectum; and 4% higher for prostate. Among Registered Indians in Canada (1991-2001), cancer death risk in Indigenous populations compared with non-Indigenous is 13% lower for lung; 8% higher for stomach; 11% lower for colorectum; and 9% lower for prostate.
Figure 1. Relative risk of cancer-specific mortality for Indigenous compared with non-Indigenous peoples by country and site. Source varies by country. See Sources and Methods.
Among females: In New Zealand (2006-2011), cancer death risk in Indigenous populations compared with non-Indigenous is 2 times higher for breast; 4 times higher for lung; 5.9 times higher for stomach; and 16% lower for colorectum. In Alaska, United States (1999-2009), cancer risk in Indigenous populations compared with non-Indigenous is 26% higher for breast; 38% higher for lung; 7.1 times higher for stomach; 83% higher for cervix; 2.4 times higher for colorectum; and 12% lower for uterus. In Australia (2012-2016), cancer death risk in Indigenous populations compared with non-Indigenous is 20% higher for breast; 2.2 times higher for lung; 90% higher for stomach; 3.8 times higher for cervix; 9% lower for colorectum; and 2.2 times higher for uterus. In the United States (2012-2016), cancer death risk in Indigenous populations compared with non-Indigenous is 30% lower for breast; 21% lower for lung; 2.1 times higher for stomach; 33% higher for cervix; and 10% higher for colorectum. Among Métis in Canada (1991-2001), cancer death risk in Indigenous populations compared with non-Indigenous is 26% lower for breast; 69% higher for lung; 66% higher for stomach; 30% higher for colorectum; and 94% higher for uterus. Among Registered Indians in Canada (1991-2001), cancer death risk in Indigenous populations compared with non-Indigenous is 14% lower for breast; 4% higher for lung; 14% higher for stomach; 53% higher for colorectum; and 46% higher for uterus.
Cancer-causing infections such as Helicobacter pylori and hepatitis B virus, which are related to poverty and overcrowding, tend to be higher in Indigenous populations, particularly in regions where vaccination for hepatitis B is not occurring. (Figure 2) Further, survival after diagnosis is lower, and its improvement is slower in Indigenous populations, suggesting Indigenous populations have not benefited equally from advances in early detection and treatment. Comprehensive, sustained efforts centered around indigenous leadership and participation are needed to improve cancer outcomes for Indigenous peoples. Cancer control planning by and for Indigenous peoples is progressing in some jurisdictions.
Figure 2. Prevalence (%) of H. pylori among Indigenous peoples, select studies. Source varies by country. See Sources and Methods.The prevalence of H. pylori among Indigenous peoples is 35% in New Zealand; 60% in Western Australia (urban); 91% in Western Australia (isolated); 78% in Alaska Natives; 67% in Canada; 47% in Greenland; and 85% in Brazil.
THE WORLD HEALTH ORGANIZATION HAS CALLED FOR THE ELIMINATION OF CERVICAL CANCER.
While disease burden is highest in lower- and middle-income countries, significant disparities exist in high-income countries. In Australia, cervical cancer incidence in Indigenous women is double that of non-Indigenous women, with mortality rates over three times higher. Strategies and actions needed to accelerate cervical cancer elimination for Indigenous women globally must be led by Indigenous women and form part of the draft global strategy tabled at the 2020 World Health Assembly.
Statistics for indigenous populations:
Personal communication from Dr. Diana Sarfati
Text:
Anderson I, Robson B, Connolly M, et al. Indigenous and tribal peoples’ health (The Lancet-Lowitja Institute Global Collaboration): a population study. Lancet (London, England). 2016;388:131–157.
Australian Institute of Health and Welfare. Cancer in Aboriginal & Torres Strait Islander people of Australia, https://www.aihw.gov.au/reports/cancer/cancer-in-indigenous-australians/contents/table-of-contents.
Sarfati D, Garvey G, Robson B, et al. Measuring cancer in indigenous populations. Ann Epidemiol. 2018;28:335–342.
Soeberg M, Blakely T, Sarfati D. Trends in ethnic and socioeconomic inequalities in cancer survival, New Zealand, 1991–2004. Cancer Epidemiol. 2015;39:860-862.
United Nations Department of Economic and Social Affairs. State of the World’s Indigenous Peoples. United Nations Publications; 2015.
Withrow DR, Pole JD, Nishri ED, Tjepkema M, Marrett LD. Cancer Survival Disparities Between First Nation and Non-Aboriginal Adults in Canada: Follow-up of the 1991 Census Mortality Cohort. Cancer Epidemiol Biomarkers Prev. 2017;26:145–151.
Figure 1:
Relative risk compares the risk of disease among people from two different groups. If the relative risk is more than 1.0, then the risk is higher. All relative risks are calculated on the basis of age-standardized rates. Age range varies slightly across studies.
Australia (2011–2015): Australian Institute of Health and Welfare. Cancer in Aboriginal & Torres Strait Islander people of Australia, https://www.aihw.gov.au/reports/cancer/cancer-in-indigenous-australians/contents/table-of-contents. AIHW. Accessed 21 Aug 2018.
United States (2012–2016): Siegel R, Miller K, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019 Jan;69(1):7–34.
New Zealand (2006–2011): Teng AM, Atkinson J, Disney G, et al. Ethnic inequalities in cancer incidence and mortality: census-linked cohort studies with 87 million years of person-time follow-up. BMC Cancer. 2016;16:755.
Canada (1991–2001, includes stomach and esophageal cancers): Tjepkema M, Wilkins R, Senécal S, Guimond E, Penney C. Mortality of Métis and registered Indian adults in Canada: an 11-year follow-up study. Health Reports. 2009;20:31-51.
Alaska (1999–2009): White MC, Espey DK, Swan J, Wiggins CL, Eheman C, Kaur JS. Disparities in cancer mortality and incidence among American Indians and Alaska Natives in the United States. Am J Public Health. 2014;104 Suppl 3:S377-387.
Figure 2:
Note: Prevalence estimates are taken from different time periods, in different population samples, and using different methods so are not necessarily directly comparable. In all cases, where non-Indigenous prevalence estimates were measured or estimated, prevalence of H. pylori was 2-3 times higher among Indigenous peoples.
Brazil (by age 8–9 years, 2007): Escobar-Pardo ML, Godoy APOd, Machado RS, et al. Prevalência da infecção por Helicobacter pylori e de parasitoses intestinais em crianças do Parque Indígena do Xingu. Jornal de Pediatria. 2011;87:393–398.
New Zealand (Pooled birth cohorts; 1926–1985): McDonald AM, Sarfati D, Baker MG, Blakely T. Trends in Helicobacter pylori infection among Maori, Pacific, and European Birth cohorts in New Zealand. Helicobacter. 2015;20:139–145.
Greenland (22–76 year olds, 1993–94): Milman N, Byg K-E, Andersen LP, Mulvad G, Pedersen HS, Bjerregaard P. Indigenous Greenlanders have a higher sero-prevalence of IgG antibodies to Helicobacter pylori than Danes. Int J Circumpolar Health. 2003;62:54–60.
Alaska Natives (prevalence by age 14 years, 1980–86): Parkinson AJ, Gold BD, Bulkow L, et al. High Prevalence of Helicobacter pylori in the Alaska Native Population and Association with Low Serum Ferritin Levels in Young Adults. Clin Diagn Laboratory Immunol. 2000;7:885–888.
Canada (prevalence by age 2 years, 1999): Sinha SK, Martin B, Sargent M, McConnell JP, Bernstein CN. Age at Acquisition of Helicobacter pylori in a Pediatric Canadian First Nations Population. Helicobacter. 2002;7:76–85.
Western Australia (3–75 year olds, 2003–4): Windsor H, Morrow S, Marshall B, Abioye-Kuteyi E, Leber J, Bulsara M. Prevalence of Helicobacter pylori in Indigenous Western Australians: comparison between urban and remote rural populations. Med J Australia. 2005;182:210–213.
Map:
The World Bank. 2015. Indigenous Latin America in the Twenty-First Century. Washington, DC: World Bank. License: Creative Commons Attribution CC BY 3.0 IGO.
Anderson I, Robson B, Connolly M, et al. Indigenous and tribal peoples’ health (The Lancet-Lowitja Institute Global Collaboration): a population study. Lancet. 2016;388: 131–157.