Management & Treatment
Existing cost-effective interventions such as surgery, radiotherapy, and access to essential oncologic drugs can greatly improve cancer survival worldwide.
Cancer management starts with obtaining a valid diagnosis. However, lack of diagnostic imaging and pathologists are major barriers to receipt of high-quality oncologic care in many parts of the world. (Figure 1) Indeed, 8 million people die annually due to poor-quality care in low- and middle-income countries (LMICs), including many due to cancer.
Figure 1. Pathologists per million population, select countries, 2011-2013. Pathologists per million population are the following: 48 in United States. 4.5 in South Africa. 2.8 in Botswana. 1.8 in Namibia. 1.4 in Kenya. 1.3 in Gabon. 1.1 in Ghana. 0.9 in Nigeria. 0.8 in Mauritania. 0.7 in Central African Republic. 0.7 in Uganda. 0.6 in Ethiopia. 0.6 in Cote d’Ivoire. 0.6 in Malawi. 0.5 in Angola. 0.5 in Tanzania. 0.5 in Rwanda. 0.4 in Burkina Faso. 0.4 in Togo. 0.4 in Zambia. 0.3 in Mozambique. 0.3 in Burundi. 0.3 in Mali. 0.2 in Democratic Republic of the Congo. 0.2 in South Sudan. 0.2 in Chad. 0.1 in Madagascar. 0.1 in Niger. 0 in Benin. 0 in Seychelles. 0 in Somalia.
Surgery is needed for 80% of early-stage cancer patients, and as a palliative measure for a substantial proportion of late-stage cancer patients. However, surgery is only delivered to one in four eligible patients globally due to infrastructure and workforce limitations, as well as lack of affordability, particularly in LMICs. Furthermore, although specialized surgery performed by an oncologic surgeon is crucial to patient outcomes, due to shortages of these specialists, cancer patients in LMICs usually receive surgery from a general surgeon. As surgery is a key contributor to improving the survival of cancer patients, the inequities in LMICs must be tackled.
The chance for a cure, the chance to live, should no longer remain an accident of geography.
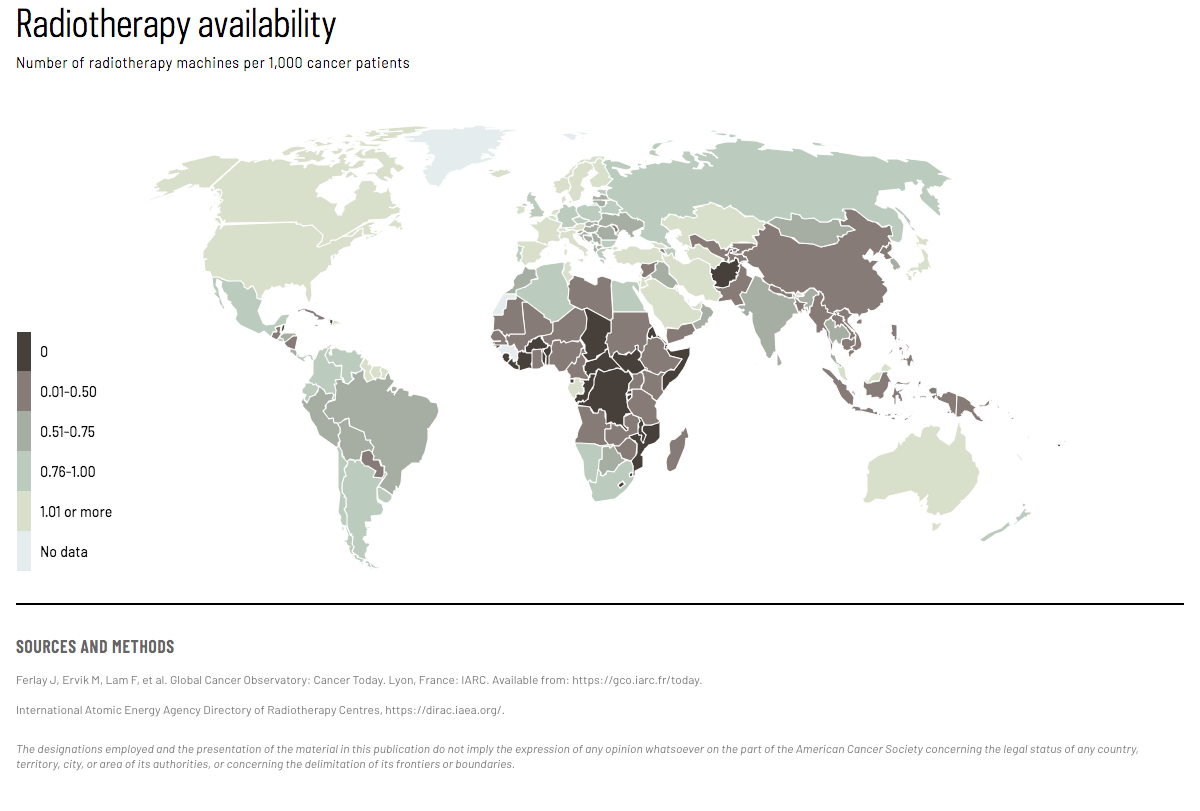
Radiotherapy is indicated for about 60% of cancer patients to cure certain tumors, relieve symptoms (palliative treatment), shrink tumors before surgery, or kill remaining cancer cells after surgery to avoid recurrence. For example, within 5 years after a diagnosis of cervical cancer, radiotherapy prevents recurrence in 1 in 3 patients and death in 1 in 5 patients. Radiotherapy coverage is less than optimal in many LMICs, with about one-third in Africa, about two-thirds in Asia Pacific, and around 90% in Europe and Latin America. (Map 1) In Ethiopia, for example, a population of nearly 100 million is served by a single radiotherapy center. Newly implementing radiotherapy (mostly in Africa) and scaling up coverage (in South-East Asia) will require financial and human resources as well as continuous technical support.
{kind=link}
Systemic therapy has changed over time, from administration of chemotherapy to all patients to personalized approaches considering receptor status, RNA expression, underlying DNA mutations, tumor environment and immunologic responses. Meanwhile, the cost of cancer drugs continues to rise, with over US$100,000 per treatment in many high-income countries. Still there are many low-cost and effective cancer drugs for broad and equitable application in LMICs, which are on the WHO essential drug list. (Figure 2, 3)
Figure 2. Breast cancer recurrence and mortality (%) with and without 5 initial years of tamoxifen treatment, 15 years after diagnosis. Among those without 5 years of initial tamoxifen treatment, recurrence was 46% and mortality was 33% 15 years after diagnosis. Among those with 5 years of initial tamoxifen treatment, recurrence was 33% and mortality was 24% 15 years after diagnosis.
Political will and stewardship at the national level, as well as greater awareness and engagement across stakeholders, are necessary to close the cancer divide. This also requires health system improvements critical to addressing the delays in diagnosis and the lack of access to therapy that lead to disparities in premature death and survival between countries. Evidence-based guidelines to perform phased implementation are provided by the National Cancer Control Network according to different geographic regions. (Figure 4)
Quote:
Knaul FM, Gralow JR, Atun R, Bhadelia A (Eds.) for the Global Task Force on Expanded Access to Cancer Care and Control in Developing Countries. Closing the Cancer Divide: An Equity Imperative. Boston, MA: Harvard Global Equity Initiative, 2012.
Text:
Abdel-Wahab M, Fidarova E, Polo A. Global Access to Radiotherapy in Low- and Middle-income Countries. Clinical Oncology. 2017;29(2):99–104.
Adesina A, Chumba D, Nelson AM, Orem J, Roberts DJ, Wabinga H, et al. Improvement of pathology in sub-Saharan Africa. Lancet Oncol. 2013;14(4):e152-7.
African Strategies for Advancing Pathology: ASAP. Available from: URL: https://www.pathologyinafrica.org/.
Davies C, Godwin J, Gray R, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771–84.
Haider A, Scott JW, Gause CD, et al. Development of a Unifying Target and Consensus Indicators for Global Surgical Systems Strengthening: Proposed by the Global Alliance for Surgery, Obstetric, Trauma, and Anaesthesia Care (The G4 Alliance). World J Surgery. 2017;41(10):2426–34.
Hanna TP, Shafiq J, Delaney GP, Barton MB. The population benefit of radiotherapy for cervical cancer: local control and survival estimates for optimally utilized radiotherapy and chemoradiation. Radiother Oncol. 2015;114:389e394.
Horton S, Sullivan R, Flanigan J, et al. Delivering modern, high-quality, affordable pathology and laboratory medicine to low-income and middle-income countries: a call to action. Lancet. 2018;391(10133):1953–64.
International Atomic Energy Agency. Directory of Radiotherapy Centres Countries report. 2019. Available from: https://dirac.iaea.org/Query/Countries.
Jaffray DA, Knaul FM, Atun R, et al. Global Task Force on Radiotherapy for Cancer Control. Lancet Oncol. 2015;16(10):1144–6.
Knaul FM, Gralow JR, Atun R, Bhadelia A (Eds.) for the Global Task Force on Expanded Access to Cancer Care and Control in Developing Countries. Closing the Cancer Divide: An Equity Imperative. Boston, MA: Harvard Global Equity Initiative, 2012.
Kruk ME, Gage AD, Arsenault C, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Global Health. 2018;6(11):e1196-e1252.
Meara JG, Leather, Andrew JM, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Int J Obstet Anesthesia. 2016;25:75–8.
Nelson AM, Milner DA, Rebbeck TR, Iliyasu Y. Oncologic Care and Pathology Resources in Africa: Survey and Recommendations. J Clin Oncol. 2016;34(1):20–6.
Robertson J, Barr R, Shulman LN, Forte GB, Magrini N. Essential medicines for cancer: WHO recommendations and national priorities. Bull World Health Org. 2016;94(10):735–42.
Shulman LN, Wagner CM, Barr R, et al. Proposing Essential Medicines to Treat Cancer: Methodologies, Processes, and Outcomes. J Clin Oncol. 2016;34(1):69–75.
Sullivan R, Alatise OI, Anderson BO, et al. Global cancer surgery: delivering safe, affordable, and timely cancer surgery. Lancet Oncol. 2015;16(11):1193–224.
Wilson ML, Atun R, DeStigter K, et al. The Lancet Commission on diagnostics: advancing equitable access to diagnostics. Lancet. 2019;393(10185):2018–20.
Zubizarreta E, van Dyk J, Lievens Y. Analysis of Global Radiotherapy Needs and Costs by Geographic Region and Income Level. Clinical Oncology. 2017;29(2):84–92.
Map:
Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: IARC. Available from: https://gco.iarc.fr/today.
International Atomic Energy Agency Directory of Radiotherapy Centres, https://dirac.iaea.org/.
Figure 1:
African Strategies for Advancing Pathology: ASAP [cited 2019 Apr 11]. Available from: URL: https://www.pathologyinafrica.org/.
Figure 2:
Davies C, Godwin J, Gray R, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011; 378(9793):771–84.
Figure 3:
Robertson J, Barr R, Shulman LN, Forte GB, Magrini N. Essential medicines for cancer: WHO recommendations and national priorities. Bulletin of the World Health Organization. 2016;94:735–742.
Explore Related Topics
This figure cannot be displayed at mobile resolutions.
To view this figure, please visit the desktop version of this website or download the PDF file of the book chapter.