Breast Cancer
Breast cancer is the most frequent type of cancer in women in almost 90% of the world's countries.
Today, breast cancer is the most commonly diagnosed cancer (27% of all cancer cases) and the leading cause of cancer death (16% of all cancer deaths) in women globally, ranking the cancer first in 158 countries for incidence and 111 countries for mortality (see Overview of Geographic Diversity). While incidence rates are highest in higher-income countries in North America, Europe, and Australia/New Zealand, the inverse occurs for mortality rates, where rates are highest in lower-income countries in Western Africa, Melanesia, Polynesia, and the Caribbean (Map 15.1).
Breast cancer incidence rapidly increased during the 1980s and 1990s in many high-income countries, driven by shifts in risk factor prevalence and widespread adoption of mammographic screening. While overall increases have slowed or stabilized in many of these countries, many countries with historically low rates are experiencing rapid increases of 3%-5% annually (Figure 15.1).
Trends in breast cancer incidence, age-standardized rate (world) per 100,000, 1975-2020
Historically high risk countries
Historically low risk countries

The trend is linked to economic growth and changes in sociocultural dynamics, leading to changes in women’s reproductive patterns (e.g., the postponement of childbearing and having fewer children) and behavioral factors (e.g., higher levels of excess body fatness and alcohol intake), along with increased detection resulting from improved awareness and diagnostic facilities. Since around the 1990s, breast cancer mortality has decreased in many high-income countries, owing to advancements in early detection and treatment. However, mortality is rising in many countries in Asia, Africa, and South America, reflecting growing incidence and an absence of the tertiary care advances seen in high-income settings (Figure 15.2). Diagnostic delays and insufficient treatment are common in many of these countries due to inherent systemic, economic, and social barriers.
Trends in breast cancer mortality, age-standardized rate (world) per 100,000, 1975-2020
Historically high risk countries
Historically low risk countries
“The success of WHO’s Global Breast Cancer Initiative will not only reduce hundreds of thousands of deaths from breast cancer each year, [but] it will also alleviate the impact of these deaths on families and on societies.”
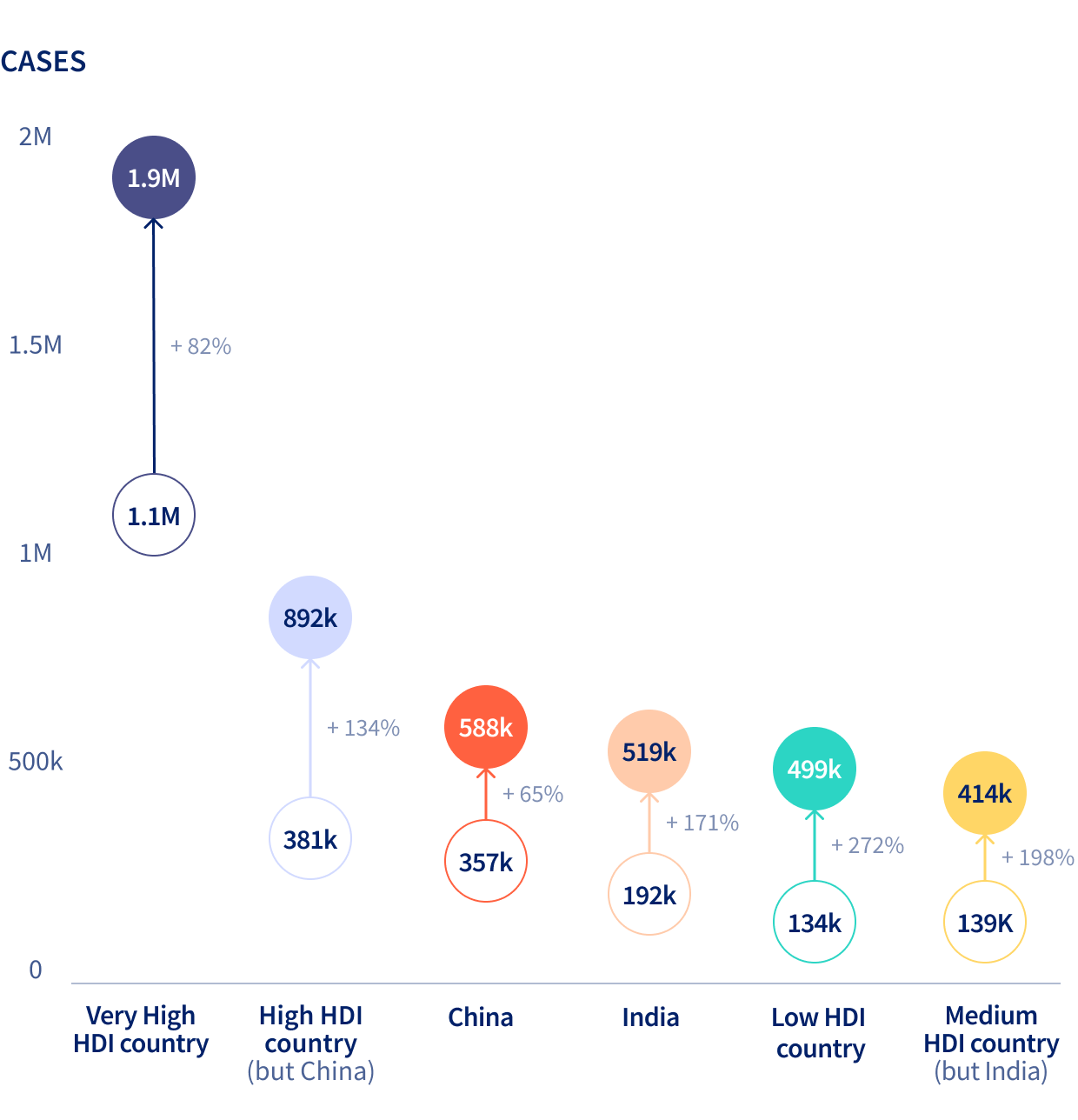
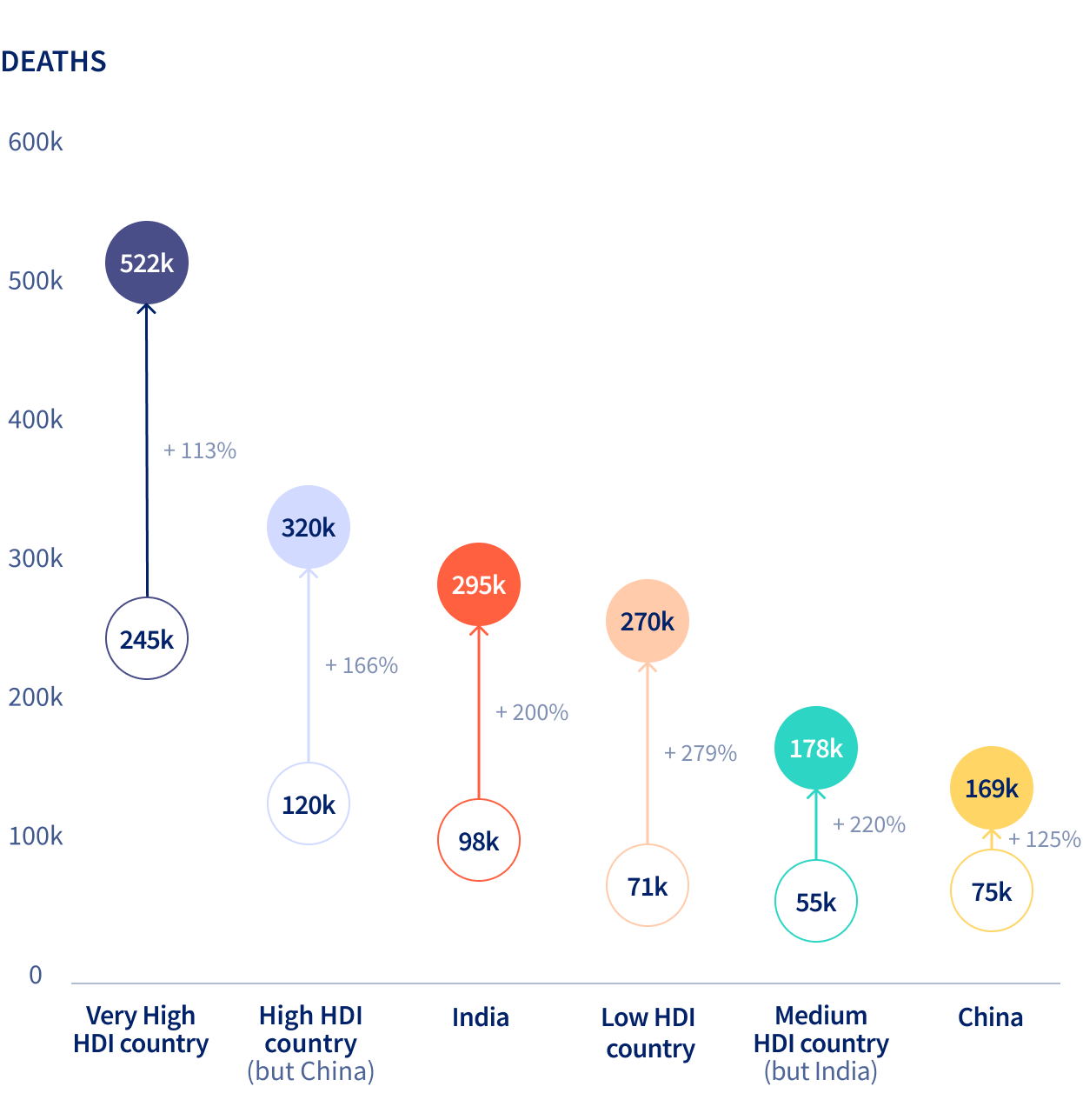
The projected breast cancer incidence and mortality burden in 2050 will impact countries in transition greatest (Figure 15.3). To strengthen systems for detecting, diagnosing, and treating breast cancer, the World Health Organization launched the Global Breast Cancer Initiative in 2021, aiming to reduce annual breast cancer mortality rates by 2.5% per year, saving 2.5 million lives over the next 20 years.
Estimated number of breast cancer cases and deaths from 2022 to 2050 by four-tier Human Development Index (HDI), China, and India